The new documentary “No Way Back: The Reality of Gender-Affirming Care” criticizes transgender ideology from a self-described “liberal, west coast Democrat” perspective. Despite facing significant resistance from trans activists, it has been making an impact.
The film will be showing in select theaters across the country during a one-day AMC Theatres Special Event on Wednesday, June 21st at 4:30 and 7:30 pm. It will be available online and on DVD starting July 2nd.
Below, Joshua Pauling interviews producer Vera Lindner.
Joshua Pauling (JP): Thanks for taking the time to discuss your new documentary. It really is a powerful depiction of what is happening to people when transgender ideology takes over. I especially found the detransitioners’ stories compelling. The story you tell throughout is decidedly reasonable and anchored to reality. Kudos to you all for producing such a thorough and moving documentary on such an important and controversial topic. And much respect for being willing to say hard but true things in the documentary.
How has the response been to the film thus far?
Vera Lindner (VL): We’ve received tons of gratitude, tears, and donations. The most humbling has been the resonance the film created in suffering parents. I wept many times reading grateful, heartbreaking messages from parents. People are hungry, culturally speaking, and are embracing our film as truth and facts, and a “nuanced, compassionate, deeply researched” project.
JP: That is great to hear, and interesting that there has been an overwhelming response from parents. Parents are frequently the forgotten victims of this ideology.
How has the film been doing when it comes to numbers of views and reach?
VL: Since February 18th, the film has been viewed 40,000 times on Vimeo, after it was shut down in its first week and then reinstated due to publicity and pressure from concerned citizens. Many bootlegged copies have proliferated on Odysee, Rumble, and such, so probably 30,000 more views there as well. After we put it on Vimeo on Demand in mid-April, it’s getting purchased about 50 times a day. Our objective is the widest possible reach.
Since February 18th, the film has been viewed 40,000 times on Vimeo, after it was shut down in its first week and then reinstated due to publicity and pressure from concerned citizens.
JP: Sad to say, I’m not surprised that it was shut down within a few days. Can you explain more about how such a thing happens? In what ways has it been blocked or throttled?
VL: Vimeo blocked it on the third day due to activists’ doing a “blitz” pressure campaign on Vimeo. Then they reinstated it, after news articles and public pressure. Our private screening event in Austin was canceled due to “blitz” pressure on the venue (300 phone calls by activists in two days). These experiences help us refine our marketing strategy.
JP: I guess that shows the power of public pressure, from either side. You know you’ve touched a nerve when the response has been both so positive as to receive countless heartfelt letters from people, and so harsh that activists want it canceled.
What do you see as next steps in turning the tide on this topic as a society? What comes after raising awareness through a documentary like this?
VL: Our objective was to focus on the medical harm and regret of experimental treatments. All studies point to the fact that regret peaks around eight to eleven years later. Yet the message of the activists toward the detransitioners is, “It didn’t work for you, you freak, but other people are happy with their medicalization.”
Our expectation is that conversations about the long-term ramifications of this medical protocol will start. We need to talk not only about how individuals are affected, but the society as a whole. Wrong-sex hormone treatment and puberty blockers lead to serious health complications that could lead to lifelong disability, chronic pain, osteoporosis, cardiac events, worsening mental health. SRSs (sex-reassignment surgeries) cost hundreds of thousands of dollars. These are not just one individual’s personal issues.
The economics of our health insurance will be impacted. The ability of these people to be contributing members of society will be impacted profoundly. The Reuters investigation from November 2022 stated that there are 18,000 U.S. children currently on puberty blockers and 122,000 kids diagnosed with gender dysphoria (and this is only via public insurance data, so likely an undercount). These all are future patients with musculoskeletal, cardiovascular, and mental illnesses for a lifetime. A hysterectomy at twenty-one can lead to early dementia, early menopause, and collapse of the pelvic floor organs.
The economics of our health insurance will be impacted. The ability of these people to be contributing members of society will be impacted profoundly.
I don’t yet see conversations about the long-term health implications of “gender-affirming care,” particularly in relation to how insurance, the labor force, interpersonal relationships, and future offspring will be affected. Everyone wants to be affirmed now and medicalized now. But there are lifelong implications to experimental medicine: autoimmune illnesses, cancers, etc. Sexual dysfunction and anorgasmia have real implications on dating, romantic life, and partnering up. A few people are talking about this on NSFW posts on Reddit.
JP: It’s interesting how speaking out against trans ideology and gender-affirming care creates some unlikely alliances across the political and religious spectrum. What do you see as the potentials and pitfalls of such alliances?
VL: We align with people who are pro-reality, who respect core community values such as truth and honesty, and who see the human being as a whole: body and soul. There is no metaphysical “gendered soul” separate from the body. Teaching body dissociation to kids (“born in the wrong body”) has led to a tidal wave of self-hatred, body dysmorphia, depression, anxiety, and self-harm. We are our bodies, and we are part of the biosphere. We respect nature and the body’s own intricate biochemical mechanism for self-regulation, the endocrine system. We believe that humans cannot and should not try to “play God.” We are students of history and know that radical attempts to re-engineer human society according to someone’s outrageous vision (read Martine Rothblatt’s The Apartheid of Sex) have led to enormous human cataclysms (communism, Chinese cultural revolution).
We are our bodies, and we are part of the biosphere. We respect nature and the body’s own intricate biochemical mechanism for self-regulation, the endocrine system.
JP: Well, then count me a realist, too! Funny you use the term pro-reality. I’ve written similarly about the possibility of realist alliances. While this makes for some improbable pairings, there can be agreement on the importance of fact-based objective reality and the givenness of the human body.
Realists can agree that the world is an objective reality with inherent meaning, in which humans are situated as embodied, contingent beings. Such realists, whether conservative, moderate, or progressive, might have more in common with each other on understanding reality and humanity than some on their “own side” whom I call constructivists: those who see the world as a conglomeration of relative meanings, subjectively experienced by autonomous, self-determining beings, who construct their own truth and identity based on internal feelings.
But I do have a related question on this point—a bit of respectful pushback, if I may.
Your pro-reality position seems to have implications beyond just the transgender question. Can one consistently oppose the extremes of gender-affirming care while upholding the rest of the LGB revolution? If our male and female bodies matter, and their inherent design and ordering toward each other mean something, then doesn’t that raise some questions about the sexual revolution more broadly?
As we see the continued deleterious effects on human flourishing unfold as thousands of years of wisdom and common sense regarding sex and sexuality are jettisoned, there are both religious and non-religious thinkers raising this question, though some go farther than others. I think, for example, of Louise Perry’s The Case Against the Sexual Revolution, Christine Emba’s Rethinking Sex, Mary Harrington’s Feminism Against Progress, and Erika Bachiochi’s “Sex-Realist Feminism.” An enlightening panel discussion with many of these thinkers was co-hosted by Public Discourse earlier this year. When the real human body is considered, its holistic structure as male or female is clearly ordered and designed to unite with its complement.
If our male and female bodies matter, and their inherent design and ordering towards each other mean something, then doesn’t that raise some questions about the sexual revolution more broadly?
How does this reality relate to the rest of the sexual revolution? If one argues that individuals should be able to express themselves sexually and fulfill their desires with no external limits beyond human desire or will, how does one justify saying that transgenderism is off-limits?
VL: I will answer the question, but I need to say that this is my personal opinion. I’m fifty-five and have worked in entertainment for more than thirty years, and in Hollywood for twenty-five years. The entertainment industry attracts LGBT people, so I’ve hired, mentored, befriended, and promoted LGBT and gender-non-conforming people every day of my career. I believe that being gay or lesbian is how these people were born. Some were affected by their circumstances, as well, but in general I believe that homosexuality is innate, inborn, and has existed for millennia. There were a handful of “classic” transsexual women as well. I have three close friends who transitioned in their late forties.
But the explosion we are seeing now is different. A 4,000-percent increase of teenage girls identifying as trans? This is unprecedented. Mostly these are autistic, traumatized, mentally ill teens who seek to belong, who wish to escape their traumatized brains and bodies, who have been bullied relentlessly (“dyke,” “fag,” “freak”) and now seek a “mark of distinction” that will elevate their social status. Instead of being offered therapy, deep understanding, and compassion for their actual traumas, they are being ushered toward testosterone, mastectomies, and hysterectomies. This is not health care. The tidal wave of regret is coming, because these adolescents were never transsexual to begin with. Many of them are lesbians or gay boys who have internalized so much homophobia and bullying that they would rather escape all of it and become someone different than deal with it.
This is what we want to address. Kids explore identities. This is a natural process of discovering who they are. Medicalizing this exploration cements this exploration they were doing when they were teens. Life is long, and one goes through many phases and many “identities.” To be “cemented” for a lifetime in the decision you made as a distressed sixteen-year-old to amputate healthy sex organs does not make sense.
JP: The rise in the rate of transgender identification is indeed stunning, as is the stark increase in the percentage of Gen-Zers who identify as LGBT. What those trends portend is a live question, as are the varied possible causes. And as you say, there is a tidal wave of regret building, from those who have been pushed toward gender transition. We will all need to make special effort to love and care for them.
You’ve been so gracious with your time. As we conclude, are there any other comments you’d like to share with our readers?
VL: Find a theater near you to attend the theatrical one-day premier on June 21st. Then the movie will become available online and via DVD on July 2nd. Watch the documentary and pass it on to all in your circles!
And ask commonsense humanistic questions:
– Can adults make decisions on behalf of kids that will forever change the path of the kids’ lives?
– Is it worth it to ruin one’s health in the name of a belief system?
– Is what you are reading in academic medical research based on evidence, or pseudo-science?
– If humans have been going through puberty for millennia, who are we to mess with that now?
– Is puberty a disease?
JP: Thank you for your work on this vital issue. I hope this documentary continues to make an impact. And realists unite!
By Borgar Jølstad and Erik Gustavsson.
Health care priority setting should be based on morally relevant factors such as need, severity, and maximizing health outcomes. But sometimes we must choose between health care allocations where these primary considerations are tied. It is sometimes suggested, and implemented in practice, that in these situations other, perhaps more controversial, factors can play the role of tiebreakers. For example, age, healthcare worker status, and first come, first serve, have been suggested as tiebreakers for ventilator guidelines in many U.S. states. This may seem an elegant solution, but tiebreakers are deeply problematic.
First, there is the issue of the value of the tiebreaker. If it is important enough to make a difference in ties, why is it not important enough to make a difference in other cases? That is, why are these factors only valuable in ties? Since any difference among the primary considerations in the priority setting system will offset the tiebreaker, any value ascribed to the tiebreaker will be miniscule. This is particularly strange in priority setting systems where ties are frequent, and the tiebreaker plays a major role in the end. The result is a minimal value making a big difference.
For example, in the Australian pandemic priority setting guidelines people are allocated to “high” and “low” priority groups based on likelihood of recovery and benefiting from treatment. Ties are to be broken by previous disadvantage and health care worker status. Presumably, the reason why these factors are ascribed the role of tiebreakers is that they are not important enough to decide whether someone is “high” or “low” priority. But strangely, they tip the scale in many cases. If a factor is important enough to make such a big difference, relegating it to the status of tiebreaker or secondary consideration seems strange.
Secondly, it is doubtful whether our reasons for implementing a tiebreaker can overcome our reasons for preferring a lottery. In Against Tiebreaking Arguments in Priority Setting we argue that lotteries are the reasonable way to break ties. Lotteries can be justified by referring to impartiality, respect for the separateness of persons, fairness, and the moral value of chances. Our reasons for preferring a lottery are particularly strong in ties, where people’s claims are, presumably, equally strong. If tiebreakers are only valuable enough to make a difference in ties, how can they overcome these reasons for preferring a lottery? Both fairness and impartiality are preserved by lotteries, whereas deciding using a tiebreaker involves allowing a professedly minimally important factor to be decisive for the outcome.
Tiebreakers are puzzling and seem notoriously difficult to justify for priority setting. If a factor is truly important, it should simply be part of our primary considerations, while ties should be decided by lottery.
Paper title: Against Tiebreaking Arguments in Priority Setting
Authors: Borgar Jølstad and Erik Gustavsson
Affiliations:
(A) The Health Services Research Unit—HØKH, Akershus University Hospital (Ahus), Lørenskog, Norway.
(B) Institute of Health and Society, Faculty of Medicine, University of Oslo, Norway.
(A) Centre for Applied Ethics, Department of Culture and Society, Linköping University, Sweden.
(B) National Centre for Priorities in Health, Department of Health, Medicine and Caring sciences, Linköping University, Sweden.
Competing interests: None
Social media accounts of post authors: @Borgar_Jolstad
The post “We could use that as a tiebreaker” – Yes, but why should we? appeared first on Journal of Medical Ethics blog.
I find the term “medical aid in dying” (MAID) deeply pernicious. It is not only an assault on human dignity (which it implicitly claims to defend), but it also employs a rhetorical sleight of hand. The term conjures up an image of someone who is already dying of a painful and terrible disease, and the aid they receive seems good and possibly even heroic. So I will switch from the misleading term “medical aid in dying” and now speak of “physician-assisted killing,” or PAK.
These misleading ideas associated with MAID have taken a firm hold of the Canadian imagination. According to a poll from Research Co., a representative sample of Canadians were asked the following question: “At this point, only an adult with a grievous and irremediable medical condition can seek medical assistance in dying in Canada. Do you agree or disagree with allowing adults in Canada to seek medical assistance in dying because of the following reasons?”
When asked about “Disability,” a full 50 percent of Canadians agreed that someone should be able to seek PAK. When breaking down the results by age groups, one might expect to find that younger folks, more attuned as they are to the nefarious effects of structural coercion, would be less likely to support PAK in the case of disability. But the opposite turned out to be the case: for 18- to 34-year-olds, support actually jumped ten points to 60 percent. In other words, 6 in 10 of young Canadians support PAK as a response to disability.
What about poverty? A lower number of Canadians—27 percent—think of it as a reason someone should be able to pursue PAK. But once again the numbers for young people are remarkable and disturbing: 41 percent of Canadians aged 18 to 34 believe it can be a legitimate reason to request PAK.
How did Canada get here? Is the United States headed down this same path? If so, how can Americans reverse course?
PAK in America vs. Canada
As families and local communities have frayed, we no longer have a ready-to-hand idea of what a good death might be apart from PAK. The dying process has been outsourced to massive, impersonal housing projects that build sterile nursing homes underwritten by vulture capitalists who discovered they can get rich on our inability to deal with death. So, to the extent that PAK gives both the dying and their families an alternative to the horror show of dying alone (except for maybe the company of a robot) in totally inadequate “care homes,” it becomes quite attractive, and pro-lifers face a serious challenge in resisting it.
Effective resistance to PAK in America has focused largely on slippery slope arguments that emphasize what happens after you open the door to this practice. If those with terminal illness can seek death, why not those with disabilities, or those suffering from severe mental illnesses? PAK opponents, in other words, are focusing on things that invoke discomfort and even anger. But will this be enough in the long run?
If those with terminal illness can seek death, why not those with disabilities, or those suffering from severe mental illnesses?
Nothing has bolstered this strategy for PAK opponents in the United States more than pointing to what is happening in Canada, whose program has expanded in ways that invoke less a slippery slope, and more a free fall accelerating at 9.8 meters per second squared. Consider that it was only five short years ago that Canada legalized PAK. And as we’ve seen, the law has recently enabled killing the poor and the disabled precisely because they are poor and disabled.
This gold-standard reporting from The New Atlantis earlier this year clearly demonstrates the extent of the horrors of Canada’s program. The program trains those who administer death to expect patients who “choose” PAK due to lacking the support they need. In a kicker that is difficult to get out of one’s mind, the article explains the message that Canada sends to its vulnerable populations:
Just a few years ago they would have been textbook candidates for what a just society would say: Your life has value. In Canada today they hear something else: Your death will be beautiful.
But what kinds of situations are we talking about? In what kinds of cases are the powers that be in Canada telling people that they might be better off dead? Well, how about a veteran who asked for PTSD treatment? Or another veteran who asked that a wheelchair ramp be built into her home? Though neither was dying, in both cases they were asked if PAK would be a better option for them.
In another case, a woman with very severe chemical sensitivities “chose” PAK after she was denied public housing that wouldn’t trigger those sensitivities. Or how about a 63-year-old man who had been waiting for spinal fusion surgery for eighteen years, and bearing terrible pain during that time, saying “I am fed opioids and left to kill myself.” He requested PAK and was approved. And then there was the 44-year-old woman with a degenerative disease who, after being denied home healthcare, decided to be as direct as she could about what actually killed her:
Ultimately it was not a genetic disease that took me out, it was a system. There is desperate need for change. That is the sickness that causes so much suffering. Vulnerable people need help to survive. I could have had more time if I had more help.
The Toronto Star, the largest and most progressive newspaper in Canada, described the move toward these practices as “Hunger Games style social Darwinism.”
PAK and Post-Christianity
Opponents of PAK in the United States have pointed to the dystopia to the north of us, and so far their strategy seems successful: even in many blue states (especially out east), PAK is not legal. Yet why has Canada gone so far with PAK? Returning to the polling figures cited at the beginning of this essay, what are we to make of these numbers in a progressive country that has adopted a position so antithetical to how Americans understand social justice?
In Canada, killing the most vulnerable human beings comports well with a society that values giving individuals what they ask for (autonomy), and a just distribution of resources (equity) in ways that allow the most people to derive the greatest benefit from them (utilitarianism).
One reason is that progressivism in the United States has retained aspects of its Christian inheritance—with its focus on nonviolence, inherent and inalienable human dignity, and preference for the most vulnerable. Progressivism in secular Canada, especially among young Canadians, is by now far removed from these commitments. Thus, in Canada, killing the most vulnerable human beings comports well with a society that values giving individuals what they ask for (autonomy), and a just distribution of resources (equity) in ways that allow the most people to derive the greatest benefit from them (utilitarianism).
It doesn’t take a genius to point out the tensions here: equity very often conflicts with utility calculations, and the poor and disabled are some of the least autonomous human beings in our communities. But that doesn’t stop the secular state, and even secular academic bioethicists in both Canada and the United States, from attempting to muddle their way through with these incoherent values in play.
The fact that increased cultural distance from Christianity may have helped pave the way for Canada’s PAK regime is further suggested by what’s happened—and what has not happened—in the much more religious United States. While Oregon and Washington (two of the least Christian states) have had legal PAK for decades, it has only recently become legal in states like California and New Jersey. And despite the best efforts of groups like Compassion and Choices (formerly the Hemlock Society), PAK is still illegal in most of the country—including in deep blue states like New York, Connecticut, and Massachusetts, as noted earlier.
The arguments that have won the day in deep blue USA are—you guessed it—about the slippery slope of such laws and the effect that they will have on the poor and disabled. Unsurprisingly, the most effective advocates against such laws are disability rights advocates (and especially disabled people themselves) who point to the disturbing data about why people seek PAK. When physical pain doesn’t even make the top five reasons people in Oregon request PAK—but fear of loss of autonomy, fear of loss of enjoyable activities, and fear of being a burden on others do make the top five—this sends a very clear message to the disabled: it’s reasonable that someone like you would want to kill yourself. And in Canada, they take the next step: we think someone like you might want to take advantage of the legal right to kill yourself.
Going on Offense
Happily, disability rights activists are still winning the day, again, even in deep blue places on the east coast. But playing a strictly defensive game of knocking down legalization attempts—especially as the United States secularizes and becomes more like Canada—seems like an untenable strategy for protecting the most vulnerable from this deadly violence. Locking in the dignity and radical equality of all human beings will require more. In short, it is time to go on offense.
A broad and diverse coalition of folks is doing exactly that: seeking to make PAK unconstitutional and therefore permanently off the books in this country. The Euthanasia Prevention Coalition in the United States recently reported on a lawsuit filed in the State of California by the United Spinal Association, Not Dead Yet, Institute for Patients’ Rights, Communities Actively Living Independent and Free, Lonnie VanHook, and Ingrid Tischer. These plaintiffs are all organizations with members who have disabilities, individual persons with disabilities, and/or organizations that advocate for persons with disabilities.
The lawsuit has the goal of reaching the Supreme Court and overturning California’s law protecting physician-assisted killing. They argue that this law is unconstitutional because it treats suicidal persons with disabilities (which according to the Americans with Disabilities Act includes those with a terminal disease) differently from other kinds of suicidal persons. If the suicidal person does not have a disability, then the state of California protects her and restricts her ability to kill herself. But if the person has a disability, then California has a special set of discriminatory rules that imply that her life is worth less and (like Canada) even refuses care and supportive services in favor of steering her toward her death. This, the plaintiffs argue, is a violation of the Fourteenth Amendment’s Equal Protection and Due Process clauses.
In my view, this a brilliant strategy on multiple levels, aligning “conservative” pro-life human dignity concerns with “progressive” disability rights concerns in a way (to this non-lawyer’s mind, at least) that makes a powerful legal, moral, and rhetorical case against legalized PAK. Again, it is long past time for us to go on offense in this battle. And the horror show we see unfolding with our secular neighbors to the north indicates just how much is at stake if we lose.
By Abeezar I Sarela.
Consent is fundamental to good medical practice. The General Medical Council (GMC) advises doctors to comply with the law in obtaining patients’ consent for medical treatment. Currently, the law on consent derives from the judgment of the Supreme Court in the case of Montgomery v Lanarkshire Health Board. This judgment emphasizes that patients require information about more than just the risks of the treatment that is proposed by the doctor. Patients also need information about ‘reasonable’ alternatives to the proposed treatment because a meaningful choice cannot be made without awareness of options.
The duty to inform patients about reasonable alternative treatments is theoretically sound but it can pose serious practical difficulties. What if a doctor considers that only one treatment is appropriate for a certain patient; and that other treatments, whilst available in general for the patient’s disorder, are not suitable in view of that patient’s particular condition? Now, is the doctor required to discuss these other treatments with the patient? There are differing views on this issue. These differences are sufficiently serious that a case was recently heard by the Supreme Court, and the judgment is awaited.
The facts of the case before the Supreme Court exemplify the problem. The patient, Mr Neil McCulloch, was admitted under the care of an acute medical team. He had pericardial effusion. The acute team made a diagnosis of pericarditis and sought advice from a cardiologist, Dr Labinjoh, who disagreed with the diagnosis. In her view, the pericardial effusion was part of some systemic disorder, with co-existent ascites and pneumonia. Accordingly, she did not advise any specific treatment for pericarditis. Mr McCullough was discharged from hospital and, unfortunately, he died two days later because of pericardial tamponade. His widow, Mrs Jennifer McCulloch, has claimed that Dr Labinjoh should have discussed the option of non-steroidal anti-inflammatory drugs (NSAIDs), which are well-established as the first-line of treatment for acute pericarditis. Her claim is supported by two experts in cardiology. But another cardiology expert disagrees. In his view, NSAIDs were not indicated in Mr McCulloch’s particular case.
At trial in the Scottish Court of Session, the judge considered whether Dr Labinjoh’s advice was reasonable by posing two questions. First, was her advice supported by colleagues in cardiology? (In legal terminology, this question is called the ‘Bolam test’). Second, was her advice logically sound? (the ‘Bolitho test’). In law, a doctor’s action is deemed reasonable if the answer is ‘yes’ to both questions. As mentioned earlier, a cardiology expert endorsed Dr Labinjoh’s advice. Also, her advice was deemed logical because, as per evidence presented to the court, the primary purpose of NSAIDs in pericarditis is to relieve chest pain; and Mr McCulloch did not have significant pain. Accordingly, the judge concluded that Dr Labinjoh had acted reasonably in not advising Mr McCulloch of the option of NSAIDs. The trial judge’s decision was upheld at appeal in the Court of Session.
The argument before the Supreme Court is, essentially, that Dr Labinjoh’s advice was not the only reasonable advice. NSAID therapy, too, would have been reasonable. Two cardiologists, who supported Mrs McCulloch’s claim, would have prescribed NSAIDs for Mr McCullough. Although he did not have a typical presentation of acute pericarditis, he did have a pericardial effusion. It was suggested that NSAIDs might reduce the size of the pericardial effusion even in the absence of pain. As such, NSAIDs were a reasonable option, and the pros and cons should have been discussed with Mr McCullough in order for him to make an informed choice.
More than one treatment may be considered as a reasonable option in many situations. But, legal analyses take place after the event. In real time, a treatment option that is considered reasonable by some doctors can seem unreasonable to others. Doctors have no way of canvassing and debating the opinions of colleagues at every step. Surely, it is each doctor’s job to use their own clinical judgment to identify reasonable options, and then involve their patient in shared decision-making about these reasonable options only. In some cases, as for Mr McCulloch, the doctor might find that only one option is reasonable.
The crux is reasonability. The word ‘reasonable’ appears 13 times in the GMC’s guidance on consent; but the GMC does not clarify the meaning of this term. The meaning remains hotly debated in political and legal philosophy. The Supreme Court’s judgment in the McCulloch case might offer some answers. Yet, it does not seem fair to expect doctors to fathom the demands of reasonability from philosophical literature and case law. The GMC should act upon the Supreme Court’s forthcoming judgment by providing some guidance on what it means to be ‘reasonable’.
Author: Abeezar I Sarela
Affiliations: Department of Surgery, The Leeds Teaching Hospitals NHS Trust
Competing interests: None declared
The post Consent for medical treatment: What is ‘reasonable’? appeared first on Journal of Medical Ethics blog.
By Adrian Thorogood and Eva Winkler.
Our paper tackles a question that policymakers and public healthcare systems are wrestling with around the world: should for-profit companies be given access to medical data derived from patients for research?
In public healthcare systems, medical data is generated as part of the routine care of patients, and through administrative processes like billing and reimbursement. Medical data is a valuable resource for research and innovation that can advance medical science and improve healthcare. Beyond academic research, for-profit companies are increasingly interested in access to “real world” medical data to inform the discovery and development of drugs, medical technologies, and data-based health applications such as AI. Many countries are actively promoting data sharing to advance public health and wealth goals.
Despite this enthusiasm, for-profit re-use of medical data from public healthcare systems continues to be a source of controversy. Hospitals and data sharing initiatives have often been criticized for a lack of transparency and social license. Some have even been shuttered or sued. Empirical surveys consistently suggest patients and members of the public are less comfortable with companies accessing their sensitive health information than healthcare professionals or academic researchers. This tension between the interests of patients and those of the public and for-profit corporations calls for a closer look at the interests of all parties involved.
Inspired by political philosophy, our paper aims to identify and evaluate the competing claims of different stakeholders relating to for-profit re-use of medical data. This includes the patients providing data, the companies seeking to use data, the society who funds and relies on its public healthcare system, and the healthcare institutions and professionals who painstakingly generate medical data.
Patients have a right to have their medical data treated with confidentiality, and a right to actively determine who accesses this sensitive form of personal data and why. Any re-use of their data should be subject to strict privacy and security safeguards, and to high standards of consent, transparency, and accountability. Patients might expect to receive a direct share in profits generated from the contribution of data. Assuming such a scheme could be practically implemented, does this claim override those of companies, hospitals and society? We argue that this is a weak claim: while medical data certainly fall under patients’ control required by the right to informational self-determination, data are generated primarily for their healthcare and no right to share in profits can be deduced.
For-profit companies in the health sector do not have a right per se to access publicly funded medical data. However, they are entitled to freedom of research – a defensive right restricting state influence on research activities – and a right to a level playing field where access is provided (non-discriminatory access). Companies do have a legitimate right to pursue and realize profits from developing high-quality, life-saving or improving health products. Where products do not offer true value, are overpriced or are not domestically available, however, commercial practices can threaten the sustainability of health systems and patient access. This seems all the more unjust for products developed using data provided by health systems and patients. As part of corporate social responsibility, companies have ethical and reputational reasons to protect patient privacy and to deliver benefits to society, reflected by the current proliferations of guidelines around responsible AI.
Hospitals and clinics are ultimately the places where patient data is generated, through the dedicated efforts of healthcare professionals and staff. Do physicians and hospital leadership own the data and have a claim to share in eventual profits? These claims are complicated by the public funding supporting healthcare delivery, patient self-determination, and the fact that data generation is only the beginning of a complex value chain. They do, however, have a valid claim to appropriate compensation for data generation and curation, one that is all too often overlooked.
Society can benefit from for-profit re-use through things like improved drug safety, as well as more accurate and cost-effective care. How can the state ensure public funds invested in health systems and data infrastructure maximally benefit society, while also maintaining public and patient trust?
Two key tensions arise: between profit maximation versus societal benefit, and between commercial and societal interests in exploiting data versus patient self-determination and privacy. To address these tensions, we conclude by suggesting conditions for ethically sound for-profit re-use of medical data:
We conclude that there are good reasons to grant for-profit companies access to medical data if they meet certain conditions: among others they need to respect patients’ informational rights and their actions need to advance the public interest in better healthcare.
Paper title: Patient data for companies? – An ethical framework for sharing patients’ data with for-profit companies for research
Authors: Winkler EC1, Jungkunz M2, Lotz V1, Thorogood A3, Schickhardt C2
Affiliations:
Competing interests: ECW and CS have been receiving grants by the German Ministry of Education and Research (BMBF) in the frame of the German Medical Informatics Initiative (MII) and have been involved in the Working Group “Consent” of the MII
The post Patient data for companies: Patient privacy, private profits and the public good appeared first on Journal of Medical Ethics blog.
By Juergen Dankwort.
The proposal to provide assistance with voluntary assisted dying (VAD) has grown significantly over the past two decades at an accelerating rate. Right-to-die movement societies and organizations now number over 80 from around the world, 58 of which are members of the World Federation of Right to Die Societies. However, most are also increasingly beset with formidable challenges opposing their advances that raise profound ethical, moral and legal considerations.
The prevalent approach towards VAD
A review of these assisted dying regimes show how they were set up through legislative acts often resulting from initial court challenges to an existing assisted dying prohibition within that country’s criminal code. They reveal a common paradigmatic model whereby the criminal act remained intact with amendments added establishing a legislated framework to allow a service under specifically designated conditions and exempting the providers from punishment.
Generally, the legal criterion for accessing such a medically-centred service requires a person to be suffering intolerably from an existing, irremediable condition defined within legislated parameters, establishing who may access them, best practices, where and when they can be done, and who may perform them.
While not alone, Canada’s often-vaunted medically assisted dying regime (also known as MAID), implemented in 2016, is exemplary of this development with attendant massive challenges facing it. Its formulation illustrates an attempt to balance a previously court-declared constitutional right to life, liberty and security of the person with a perceived societal harm resulting from a state-sanctioned service to assisted dying.
Such legislated regimes have since been challenged legally numerous times by persons refused access, while featuring alarming stories in the media when access was sought and granted. A backlash to VAD has gained recent traction.
Traditional assisted dying opponents, including the orthodox religious, some disability groups, and conservative politicians who often troll to their populist base, are joined by additional academics and some physicians, providing more legitimacy with compelling arguments at stopping any wider access to a state-initiated and financially-covered national health service.
Germany breaks tradition
In a remarkable judgment by the German Federal Constitutional Court in February 2020, regarding assisted suicide, a ground-breaking option for any country or jurisdiction contemplating the creation of an assisted dying regime was identified that may well avoid much of the controversy and many of the challenges faced by existing ones. It does so by revealing a pathway to set up the service based on an entirely different orientation and approach from the existing one that began decades earlier in Europe, and later largely copied by others.
The German Court’s ruling stated for the first time that matters of quality of life and degrees of suffering are wholly subjective and that governments should therefore not prescribe nor proscribe assisted dying access based on categories of populations defined by such individually-experienced life-determinants because such restrictions would violate entrenched principles regarding personal autonomy and the liberal foundation separating state and personhood in pluralist societies. A VAD regime built on this premise could then also avoid all expressed objection to assisted suicide, no longer based on those normative criteria.
A recent study out of Europe contrasting two ways of how assisted dying services function, detail the actual process deciding for whom and when the service may be administered and who can perform it. The legislated regime of Belgium – a model used for Canada’s – was compared with the process in Switzerland.
Importantly, no legislated system was erected in Switzerland that specifies through amendments or exceptions how, when, by, and for whom it may be done. It has remained unlawful for decades with the simple caveat if it is done to exploit another vulnerable person. Several salient differences were observed by the researchers that also reveal the challenges presently facing existing VAD regimes. The Swiss model featured:
While claims that Canada has become the wild west for assisted dying with catastrophic consequences is arguably exaggerated given its stringent access requirements, it is nevertheless exemplary of a heightened political drama resulting from the path it took historically that set it on its stormy course.
That begs the question if the many countries and jurisdictions now considering a VAD gateway might not consider taking a different route illustrated by the current Swiss way, recently given a legal foundation by its European neighbour.
Though convincing evidence is still lacking on how expanding assisted dying allegedly leads to a slippery slope of harming the most vulnerable, as reported by some right-to-die societies and as shown in studies, opposition and barriers to it will likely invite more impulsive, desperate suicides that may traumatize and endanger friends, family, and first responders.
Author: Juergen Dankwort
Affiliations: Associate, University of West Virginia Research Center on Violence
Competing interests: Member, Right to Die Society of Canada; Supporter, World Federation of Right to Die Societies; Coordinator, Canada chapter, Exit International.
Declaration:
The author was not paid by any organization, group, government or individual in conducting research for and writing this article.
The post Overcoming impediments to medically assisted dying: A signal for another approach? appeared first on Journal of Medical Ethics blog.
By Daniel Sokol.
A patient presents to the colorectal clinic with bleeding from the rectum. “Doctor”, he says sheepishly, “I must tell you that I have sex with my dog.”
Intercourse with an animal, once known as ‘buggery with an animal’, is a criminal offence under s69 of the Sexual Offences Act 2003, with a maximum penalty on conviction of 2 years’ imprisonment. The offence covers both the intentional penetration of a living animal’s vagina or anus with the offender’s penis, or intentionally causing or allowing one’s anus or vagina to be penetrated by the penis of a living animal.
Should the doctor breach the patient’s confidentiality and inform the relevant authorities?
The duty of confidentiality appears in the Hippocratic Oath and has been described by the 17th century French doctor, Jean Bernier, as the “soul of medicine”.[i] The French call it “le secret médical” (“medical secret”), stressing the link between secrets and confidentiality. There is a strong public interest in the maintenance of this duty. Without it, the all-important trust between doctor and patient will be eroded. Patients may be reluctant to share private information with their doctors, or may not attend their doctor at all, with adverse consequences to their health. Would this patient have spoken so freely without a belief that the doctor was duty-bound to keep his secret? Maintaining confidentiality may therefore benefit the health of the patient and, more broadly, society.
Yet, however strong, the duty is not absolute. There are times when a doctor must, by law, disclose a patient’s information, as in the case of certain notifiable diseases and under terrorism legislation.
In this case, the doctor is under no statutory obligation to breach the patient’s confidences. The question is whether the doctor may do so in the public interest. There is, in my view, such an interest in protecting a dog from the likely harm, whether physical or psychological, of sex with a human and bringing offenders to justice.
On the other end of the scales, aside from the public interest in preserving a strong duty of confidentiality, must be placed the patient’s potential harm or distress from the disclosure, including the loss of his liberty in the event of a custodial sentence, financial loss if fined, and the loss of trust in the medical profession. In my experience, patients whose confidentiality has been breached regard it as a betrayal, a break of an implicit promise of secrecy, and develop an antipathy to doctors.
In its guidance, the General Medical Council permits disclosure of confidential information if this is likely to be necessary for the prevention, detection or prosecution of “serious crime”. There is no definition of this term, although there is specific mention of crimes against the person. While offences such as murder, manslaughter, rape, kidnapping, child abuse, and grievous bodily harm would plainly fall within the category of serious crime, it is doubtful that intercourse with an animal, whose ordinary sentence would result in a community order rather than imprisonment, would so fall. The Department of Health’s supplementary guidance on public interest disclosures, published in November 2010, noted that a serious crime will “likely include…crimes which carry a five-year minimum prison sentence but may also include other acts that have a high impact on the victim.”
In my opinion, faced with this ethical conundrum, the doctor should have sought advice from colleagues, the Trust’s ethics committee, their defence organisation, or the British Medical Association’s ethics hotline, to help conduct the balancing exercise above. If consulted at the time, I would have advised the doctor to maintain the patient’s confidentiality. The public interest in disclosure does not appear compelling enough to tip the scales away from the strong Hippocratic duty to keep the patient’s secrets.
The doctor should nonetheless advise the patient of the medical risks of his sexual activity and recommend referral to a mental health professional.
[1] Bernier, J. Essais de médecine (Paris, Simon Langronne, 1689), p.268
Author: Daniel Sokol
Affiliations: 12 King’s Bench Walk Chambers, London, UK; medical ethicist
Declarations: This article does not constitute legal advice and should not be used as a substitute for such advice.
Competing interests: None declared.
Social media account of post author: @DanielSokol9; Website
The post To breach or not to breach a patient’s confidentiality? A case study in the colorectal clinic appeared first on Journal of Medical Ethics blog.
Written by Rebecca Brown
This post is based on two recently accepted articles: Brown and de Barra ‘A Taxonomy of Non-Honesty in Public Health Communication’, and de Barra and Brown ‘Public Health Communication Should be More Transparent’.
In a previous post, I discussed some of the requirements for public health institutions to count as ‘honest’. I now want to follow that up to discuss some of the ways in which public health communication seems to fall short of honesty.
I’ll follow Christian Miller’s definition of the term ‘honesty’ to refer to a character trait that involves being disposed, centrally and reliably, to not intentionally distort the facts as one sees them. As discussed previously, it is pretty hard to get at the intentions of agents. We can rarely – if ever – say with certainty that a particular agent intended some outcome, since that information is available only to the agent herself. Instead, we must rely on extrapolating from whatever evidence is available to us.
This can make it hard to prove a failure of honesty, since we must often rely upon a ‘best guess’ as to the agent’s motivation when they acted in a particular way. For the kinds of cases I’m interested in – communications from public health organisations – it is even trickier, as it is not clear what agent is responsible for the communicative act in question (it could be an individual within an organisation, the organisation itself, or some subset of the organisation/individuals within it). But assuming certainty isn’t required, we might still judge that an agent (group or individual) probably intended to mislead or otherwise distort facts if the way they presented information could reliably be expected to create false beliefs in the recipient, and if we would reasonably expect the communicator to have known this. With that in mind, we might speculate about the honesty or otherwise of public health communication.
Public health communication frequently engages in a number of practices that look like they might not meet the demands of honesty. Some examples are:
Magnitude neglect where public health communication doesn’t provide an indication of the expected effect size of the benefit / harm discussed. This could include, for instance, saying that screening reduces your chance of dying from cervical cancer, without telling you by how much your risk of death is reduced.
Harm neglect involves providing information about the benefits of recommended behaviour changes / interventions without mentioning any possible harms.
Relative over absolute risk presentation. Whilst communicators rarely provide quantified effect sizes of the benefits associated with a recommended behaviour, when they do provide such estimates they often use relative risks rather than absolute risks. This will tend to inflate people’s estimate of the size of the benefit they can expect. For example, an intervention that reduces your risk of developing diabetes from 0.001% to 0.0005% cuts your risk in half – that is, reduces it by 50%. The first way of presenting this (using absolute risks) makes the change seem quite small; the second way (in relative risks) makes it seem much bigger. Public health communicators will often use relative risks to describe health benefits, which tend to make them seem much more impressive.
Mismatched reporting takes the above tendency, and pairs it with a tendency to report the harms of recommended behaviours in terms of absolute risks. If relative risks inflate people’s expectations, absolute risks deflate them. Pairing benefits described in relative risks with harms describes in absolute risks seems geared to encourage people to overestimate benefits whilst underestimating harms.
Causation laundering occurs when the content of public health communication implies a causal link between phenomena when it is difficult to know to what extent the relationship is causal. For instance, the health benefits of exercise are widely proclaimed (the NHS describes it as a “miracle cure”. Yet it is very difficult to extrapolate what health benefits associated with exercise are a result of exercise making people healthier, and what results from healthier people doing more exercise. Public health communicators sometimes gloss over such ambiguity, and imply that the causal relationship acts only in one direction – that is, exercise causes good health, rather than the other way around.
These ways of communicating health information, amongst others, seem likely to encourage people to form overoptimistic beliefs about the benefits of various health behaviour changes. Moreover, this seems predictably likely and – we might speculate – intentional. If this is indeed the case – if public health communicators intentionally frame their messages so as to encourage people to form overly optimistic (and inaccurate) beliefs about the likely benefits of health behaviour change – then this is inconsistent with communicating honestly.
This leaves out the question of whether or not there is anything wrong with failing to communicate honestly. Whilst there will almost certainly be cases where honesty is not all-things-considered desirable (e.g. it is better to tell a lie to protect an innocent victim from a murderer than to tell the truth and condemn them to death, contra Kant) it is not clear that public health communication is typically one such case. Indeed, it seems unlikely, given the emphasis on honesty in clinical communication, and the importance of allowing people to make well-informed decisions about how to lead their lives and take care of their health.
Most of the behaviours considered here – relating to diet, exercise, cancer screening and other preventative behaviours – require people to forego pleasures in the pursuit of longer term health. Whilst public health professionals might emphasise that there is “no safe” drinking level, individuals might reasonable decide that the benefits of alcohol consumption outweigh the risks. But people can only make these decisions sensibly if they are accurately informed about the harms and the benefits of these behaviours. And this requires public health communication to give a non-distorted, honest, picture of the available evidence.
References
Brown and de Barra (in press) ‘A Taxonomy of Non-Honesty in Public Health Communication’ Public Health Ethics
de Barra and Brown (in press) ‘Public Health Communication Should be More Transparent’ Nature Human Behaviour
Miller (2021) Honesty: The Philosophy and Psychology of a Neglected Virtue, Oxford University Press
By Abeezar I. Sarela.
In its recent guidance on consent, the General Medical Council (GMC) advises doctors to not provide treatment that ‘you (the doctor) don’t think would be in their (the patient’s) clinical interests’. It follows that doctors should only provide treatments that are in the patient’s clinical interests. But, what exactly is meant by ‘clinical interests’?
The GMC does not explain the term. In practice, it is sometimes confused with ‘best interests’. However, best interests is a legal term that applies specifically to making decisions for people who lack the capacity to do so for themselves. For example, oncologists might consider that either chemotherapy A or chemotherapy B could be in the clinical interests of a patient without capacity. Best interest decision-making would then involve choosing between A and B, or avoiding any chemotherapy and giving supportive care only. Whereas, patients with capacity would make these choices for themselves and do not need others to decide their best interests.
The difference between clinical interests and best interests is similar to that between setting a menu and then choosing from that menu. Clinical interests set the menu of treatment options that is available to a patient. Patients can then choose any option from this menu or decline all options, regardless of the consequences, because we all have a right of self-determination. But, do patients have a right to participate in setting the menu, too? Some might say yes. They would argue that treatment availability comes down to a matter of informed consent, through a process of shared decision-making (SDM) between the doctor and the patient.
However, senior judges have been clear that consent is valid only if the proposed treatment is, in the first place, ‘proper’. If the treatment is not proper, then the patient’s consent is meaningless, regardless of the sharing of information. In other words, setting the menu is not a matter for SDM. Rather, informed consent has two distinct stages. In the first stage, the doctor has to identify treatments that are proper (reasonable or available) for that patient. Then, the doctor has to involve the patient in the choosing between available treatments (or not having any treatment). It is this second stage that requires SDM: a dialogue about the menu of available treatments from the first stage.
What is it that makes a treatment available in the first place? Judges have explained that for a treatment to be available it has to be in the ‘public interest’. This turn to public interest can be justified in various ways. In a civilised society, we all (the ‘public’) have an interest in each other’s welfare. And, in some cases, the public interest can override an individual’s own wishes. Furthermore, in a publicly-funded health service it is inescapable that making treatment available to one person reduces resources for others. Consequently, it is in the public interest to set limits on availability of treatment.
The GMC would seem to have re-phrased ‘public interest’ as ‘clinical interests’. The endpoint of both is the same: the identification of available treatments. Thus, in advising doctors to think about a patient’s clinical interests, the GMC is actually asking doctors to consider the public interest. The GMC leaves this task to the professional judgment of doctors; and judges have done similarly. This approach is consistent with a well-established sociological argument that the public grants the medical profession with the authority to make certain decisions on its behalf. As doctors, let’s celebrate this sociological mandate and strive to serve the public. Or let’s challenge it, and find an alternative way. But, in the meanwhile, let’s not hide behind smokescreens of SDM and consent to decide about the availability of treatment.
Author: Abeezar I. Sarela
Affiliation: Department of Surgery, The Leeds Teaching Hospitals NHS Trust.
Competing interests: None declared
The post Re-thinking consent for treatment: clinical interests and the public interest appeared first on Journal of Medical Ethics blog.
By Nathan Hodson.
It is late evening on an acute psychiatry ward and I’m the on-call doctor responsible for clerking a new patient with acute psychosis. I look in the notes and see that despite a history of detention for paranoid schizophrenia, he has been well on an antipsychotic depot for 5 years. Why relapse now? Then I find the most recent letter and discover that he stopped accepting his depot two months ago and rapidly declined. This terrible pattern is a common occurrence in acute psychiatry. Patients are deprived of their liberty and detained under the Mental Health Act because of depot non-adherence. Financial incentives may be one way to address this problem but progress has been slow.
Two medium-sized RCTs have shown that adherence to antipsychotic depot injections is improved when patients are offered a small financial incentive (worth roughly 2 and a half hours at the minimum wage). These studies are conducted among patients who have discussed depot treatment and agreed to it but are at risk of missing doses perhaps due to distractions or inconvenience. Nevertheless, a range of ethical and practical issues have been raised in empirical and philosophical studies. These questions are fascinating and important and while there are some answers emerging from the literature, many questions have not been fully addressed. We catalogued the full range of published objections in our recent systematic review.
Some claims about financial incentives for antipsychotics are difficult to evaluate because there is no useful data. For example, we do not know whether incentives improve mental health outcomes, reduce hospitalization, or benefit patients with good compliance. There have been no studies comparing different incentive designs despite extensive evidence that different incentive designs have different results. Similarly, there is no evidence whether incentives mean patients explore their options less assiduously or hide adverse effects. Overall there is no useful evidence regarding cost effectiveness.
However, many questions which have been raised about financial incentives have been answered by empirical study. Can incentives increase depot adherence? Yes (in both RCTs). Can they increase overall engagement with treatment? Yes (44% of the time). Can they upset patients not offered incentives? Occasionally (one report of a patient missing a dose in protest from all studies so far). Does withdrawing incentives undermine intrinsic motivation and adherence? No (no difference between incentive and control group in intrinsic motivation). Will patients become financially dependent? No (not reported in any study so far).
But we also identified certain objections that were simply not amenable to direct empirical study. These included impact on patient dignity and autonomy, coercion, exploitation, and disrespect for settled decisions. These questions require philosophical research with empirical scaffolding.
Interestingly, a key part of that empirical scaffolding already exists. Our new paper Take patients seriously when they say financial incentives help with adherence reviews evidence to support the simple but important observation that patients view incentives favourably. Compared to mental health staff, patients are much more positive about incentives. They report that they enjoy having extra money. They dislike the idea of non-cash incentives. Altogether, patients are – and it is not surprising in retrospect – hugely positive about receiving some spending money for doing something they were probably going to do anyway. It is striking that mental health staff (just like me and my colleagues) overlooked this benefit
Patients also took a surprising moral view. Unlike mental health staff, they endorsed the idea that financial incentives are an appropriate reward for good behaviour and that, in this case, accepting their antipsychotic depot constitutes good behaviour. This view is more in keeping with Kohlberg’s preconventional stage of moral development where people are driven by reward and punishment. I think many ethicists would balk at this particular justice-based argument for incentivising people to accept treatment which is their best chance at staying well and out of hospital.
But in another sense, many of us view healthy actions as morally good. Working out, staying hydrated, avoiding sugary foods – we attribute moral value to them all. Does that mean we should all get incentives? Maybe not. But it does explain why incentives make sense to patients with schizophrenia. We could construe such incentives as celebrations or well dones. The fact that this view seems to be meaningful to patients perhaps suggests ethicists have overlooked a very simple dynamic in the relationship between psychiatrists and psychotic patients and the exact meaning given to any financial incentive.
It is nice to receive a celebration, or acknowledgement, that you have done something good. Evidence given by patients reveals a positive regard for incentives and this perhaps surprising ethical interpretation. In light of these findings, it becomes more difficult (although not impossible) to make the case that incentives are problematically paternalist or coercive. I suggest that these surprising findings do, however, make a prima facie case for further research into financial incentives for depot antipsychotics as one means of reducing psychotic relapses like the ones I see in hospital. The onus is on opponents of financial incentives for antipsychotic treatment to present arguments which outweigh patient preference.
Author: Nathan Hodson
Affiliations: Academic Clinical Fellow, Unit of Mental Health and Wellbeing, Warwick Medical School
Competing interests: None
Social media account of post author: @nathanhodson
The post Have ethicists overlooked obvious benefits of financial incentives for antipsychotics? appeared first on Journal of Medical Ethics blog.
By Anna Nelson.
Prompted by a sensationalist headline in the Daily Mail, there has been a furore on social media around an article published last year by bioethicist Anna Smajdor in which she defends ‘Whole Bodily Gestational Donation’ (WBGD). Put simply WBGD means that, with prior consent, the bodies of women in a permanent vegetative state could be used to gestate pregnancies on behalf of others.
The purpose of this blog is not to engage with the ethics of this proposal, nor is it to suggest that the paper on WBGD ought not to have been published (on this latter point, see J.Y. Lee). Rather, this blog reflects upon the widespread public response to the media reports on Smajdor’s article, and suggests that some of this anger could be more usefully focussed on present day challenges which threaten the rights and safety of women and birthing people.
Understandably, many of the concerns raised by social media users in response to WBGD were explicitly feminist in nature and highlighted worries about potential harm to women – physical harm to the bodies of the donor, harm to reproductive and bodily autonomy where coercion or lack of information undermines consent to such procedures, and broader, socio-cultural harm attached to the risk of WBGD compounding and perceptions of women as foetal environments.
I am not looking to address the legitimacy of such concerns, nor do I question people’s right to express these. Rather, I question why a theoretical exploration of a speculative aspect of reproductive science has attracted so much more attention and outrage – both by those in the media, and by those responding on social media – than the very real and very present way that women and birthing people are being harmed by the current under-investment in maternity services. I argue that those of us who are rightly worried about the way that future scientific developments could interact with society and medical institutions to sustain and perpetuate harm to women, need to have (at least) equal concern for that which is happening right now.
The disparity in outrage was powerfully illustrated by the fact that, only four days after WBGD came to widespread public attention, a shocking and heart-breaking story was published on BBC News, outlining how delays in post-birth treatment and poor interpretation services may have contributed to the post-partum death of a woman in Gloucester. While it would be inaccurate to suggest that this story went unnoticed, it received only a fraction of the attention that was prompted by Smajdor’s theoretical paper – both from the media and from the wider public.
This incident was not an isolated tragedy. Last year saw the publication of the final Ockenden Report on the independent investigation into maternity services at Shrewsbury and Telford Hospital NHS Trust, and the Kirkup Report on the independent investigation into maternity and neonatal services in East Kent. In both instances it was concluded that serious failings had resulted in avoidable harm to birthing women, their babies and their families.
Particularly shocking was the evidence laid out in the Kirkup Report about the “basic lack of kindness, care and understanding” being shown to “women and their families” (p48) and the failure to “ensure or preserve women’s dignity or meet their basic needs” (p50). Alongside this, both the campaign group FIVExMORE and the charity Birthrights published damning reports which highlighted the physical and psychological harm caused by systemic racism within the maternity services:
“There was one point in my labour right near the end where I remember looking at [my Partner] and saying, I’m going to be a Black statistic. I was so scared, and the epidural hadn’t come so I felt like people weren’t listening to me, it had been days…’
These reports clearly demonstrate that feminists are right to worry about the harms faced by women in the reproductive sphere – be those harms to physical safety, to bodily autonomy, to dignity or to psychological wellbeing. Yet, none of these issues attracted nearly as much attention or widespread public outrage as the theoretical discussion of WBGD. This, I suggest, illustrates that the groundswell of anger which was seen on social media following news coverage of Smajdor’s paper was somewhat misplaced; as reports about the ongoing, harmful experiences of women and others who birth within the current system do not attract the same levels of attention and public comment.
Of course, we should debate future scientific developments before they come to pass, and of course it is vital that we parse the potential intended and unintended consequences thereof (as someone whose PhD looked at partial ectogenesis, a speculative reproductive development, it would be incredibly hypocritical of me to suggest otherwise!). However, it is imperative that the same scrutiny is applied to the less sensational but arguably more materially significant harms which are experienced by women and birthing people, and their families, every day as a result of a maternity system which is underfunded, understaffed and undervalued.
While advances in reproductive science and technology do carry the potential to create new harms, it is more likely that they will serve to compound and magnify existing problems. Therefore, when we are thinking about these developments it is important not to lose sight of the forest for the trees. In order to truly protect women (and others who gestate), it would be helpful to direct some of the very vocal anger which was whipped up by Smajdor’s paper towards the very present and pressing fight to fund and sustain a maternity system which centres the dignity and safety of all who birth.
Author: Anna Nelson
Affiliation: Centre for Social Ethics and Policy, Department of Law, University of Manchester
Competing interests: None declared
Social media account of post author: @Anna_Nelson95
The post The furore around whole bodily gestational donation: a tale of misplaced anger? appeared first on Journal of Medical Ethics blog.
In today’s interview, Leah Libresco Sargeant speaks to Dr. John Bruchalski. He is an OB/GYN based in Virginia, and the author of the recent memoir Two Patients: My Conversion from Abortion to Life-Affirming Medicine. Sargeant is the creator of Other Feminisms, a substack focused on the dignity of mutual dependence. Their conversation has been edited for length and clarity.
Leah Sargeant: Dr. John Bruchalski, you’re an OB/GYN who used to practice what people would think of as the full spectrum of obstetrics and gynecology, including abortion. And that’s something you chose to walk away from.
I want to ask you a little bit about that choice and about what your new practice looks like, starting with one of those pivotal moments you described in your book when you went into the operating room for an abortion and were confronted by a baby. Can you tell me about that night?
Dr. John Bruchalski: At that point, I’m working at a pregnancy center at night, but during the day, I am doing the full spectrum of OB/GYN, including aborting healthy children, sick children, just about for any reason at any time. Abortion on demand.
And that dissonance is becoming more and more tense for me.
So there I am in one room saving a 22-weeker because the mother desperately wanted it. She’s praying, she’s begging, she’s imploring. We have her in Trendelenberg [a position to forestall premature labor], kind of tilted backwards. We’re using medication and antibiotics, and she’s getting better.
In the other room, mom didn’t want it. She’s like, “No, just get rid of it.” And what did I do? I broke her water and pitted out the baby [administered Pitocin to induce labor].
Now the baby comes out and I lift it. And usually when a baby’s born alive in an abortion, we suffocate it [by not assisting breathing].
But it felt a little heavy. I threw the baby on the scale and lo and behold, 505 grams [over the legal limit, requiring life-saving treatment], I had to call the intensive care nursery. In walks Dr. Debbie Plum [from the NICU team], she takes one look and says, “Hey John, you’re better than this. Stop treating my patients as tumors.”
This baby weighed about a pound and a quarter. Its skin was translucent. It made noise, it was obviously human, part of our family. But the dissonance is: no, call it a fetus, it’s not wanted.
It’s unwanted. So therefore we need to terminate it. The mother doesn’t want it, society doesn’t want it.
LS: I was really moved reading your story of that night and that delivery. I went and looked up kind of what that critical threshold was for the baby. And it was five grams, you said, over the limit.
And so I looked up, what else is five grams? A sheet of paper. A sheet of paper weighs five grams. And that was the measure of what made someone a person or not in the hospital.
JB: That’s exactly right. Once you remove medicine from truth and justice and equality and equity and ecology, five grams—a sheet of paper or whatever the mom wants. It’s a desire.
I began to see my heart hardening as I was doing more and more abortions. You go from the little ones that have no bones to the ones that have bones, and eventually you realize something’s not right here. You think now it’s human, at one point it wasn’t. But no: I later realized that if mom and dad give us the egg and sperm, it’s a human life. Period.
LS: I want to dive in on that shift in vision. I think of these arbitrary thresholds (five grams, one more week) as the things that mark the change from objects to persons. And these thresholds are particularly painful in the context of abortion, but they’re also problems in a lot of places in medicine.
For example, doctors might say: “Oh, you’re not quite sick enough for a transplant. But once your numbers move by 0.1 on this scale, we’ll be able to treat you differently.” And I know that in some cases those numbers come out of a real place of care, of we have to make these decisions based on aggregate data. But as a doctor, how do you balance “These numbers tend to work overall,” and “I have a single patient in front of me I want to advocate for?”
JB: You always hate the disease, but you always love the patient. That’s the core of medicine.
For instance, the thyroid gland has a normal range, but that normal range is based on an aggregate, it’s not your range. So in my practice, one of the ways I’ve done this just in medicine is if your TSH is above a two, it’s telling me that it’s working too hard.
Because we’ve been a part of eugenics and a part of destroying the weak forever, there’s a dark side to medicine that you really have to be careful about. There’s a better way to practice.
Well, why not try a little bit of supplementation or kelp or iodine? You have to look at the individual person and listen to her story. And that’s what happened that night when I tried to kill that baby. She was further along than I thought. Once you start becoming callous to human lives, it becomes a calculus: put in the numbers. You meet the bar. I’m convinced it’s like the train platform at Auschwitz-Birkenau. You go here, you go there based on some line drawn between human and non-human. Some people are part of the human family and some are not.
And I think medicine, because we’ve been a part of eugenics and a part of destroying the weak forever, there’s a dark side to medicine that you really have to be careful about. There’s a better way to practice.
LS: I appreciate that, especially because I think this is an issue, again, that’s certainly in stark relief in obstetrics and abortion, but it’s not limited there. I got a quote from the book here.
“We were taught to trust our patients above all else. And for whatever reason, this woman felt the abortion would make life better. It wasn’t my place to question her choices. I was there to help women.”
And I can tell that your practice is moved by love in both cases when you were providing abortions, now when you’re eschewing them.
But there’s also this pressure from the medical system that the doctor is a vending machine, that you’re there to provide a service. And that’s not limited to abortion. So how do you resist that vending machine pressure, even in a pro-life practice? Where does that pressure come from?
JB: Modern bioethics is based on patient autonomy. I don’t do abortions anymore because they’re not good for unborn, the most weak. But it’s also not good for families or moms, psychologically, medically, that sort of thing. Or even for me as the abortion provider: I’m still post-traumatic. It was part of my life.
When I became this holistic, integrated, life-affirming doctor, I will try many alternatives to see where the data leads us. And you realize that when you listen to your female patients, they are live books.
LS: I like that metaphor because I’ve been in the position where it feels like I have to advocate for myself against a doctor. And so I’m sympathetic to someone who feels like they’re coming in to try and kick the vending machine to get the treatment to come out.
I think good medicine relies on a trust that isn’t there for many patients with their doctors or for doctors with their hospital system, at every level. That lack of trust is part of why people are so skeptical about the possibility that there’s a way to treat both patients; instead, they expect it to be a zero-sum game.
When you look at the statistics on maternal mortality in America, it’s clear many doctors aren’t treating both patients. They may be shortchanging mother and child, but it’s clear moms are getting shortchanged. The most famous recent example was Serena Williams, a famous woman, an important woman, a rich woman having to drag herself off her hospital bed to beg to be checked for a condition she knew she had that was putting her in danger of death.
And when I see those stories, I understand why people who are pro-choice and who care about women say, “I don’t trust the pro-life movement to write laws that won’t leave women in trouble, even if hypothetically it’s possible to do perfect practice.”
I’m going to give you a specific example: imagine a woman who comes in with premature rupture of membranes at 19 weeks. Is it possible to take care of her and the baby? Certainly. Do they expect the doctor is going to do it? No.
So how do you respond to that lack of trust where it’s possible to practice medicine, in a way that woman and baby are taken care of, but manifestly we don’t? How do we advocate a system of laws that puts the appropriate weight on the baby’s life when we know we don’t put that weight on the mother’s life, even in an uncomplicated delivery?
JB: I have to be honest with you, that’s a very hard question because “the life of the mother” exception is a political reality. It’s not scientific.
The only way that you can regain this trust, I believe is not politically, it’s actually by witnessing. So Tepeyac OB/GYN and Divine Mercy Care, what we do now is just out there trying to respond to this question that you ask me. In our practice at Tepeyac, we probably have eleven women whose water broke at 15 weeks. And they all delivered children over 34 weeks.
LS: How do you have a conversation with a mom in that position about what the risk is like? Because I think that risk really worries people.
JB: You can tell a mom in that position that the world literature that has researched water breaking early says you should be able to wait. It says you have to monitor her very closely, along with following her baby. So I tell these moms that we’re going to be taking her temperature every day, morning and night. And by monitoring them closely, we will deliver you as soon as there’s any sign of infection. Because if there is, we then target the infection, not the baby.
You would never tell her, “Well, I’m going to kill your baby to save your life because you might die of an infection.” That’s bad medicine and bad anthropology. In our practice, sometimes this decision to keep monitoring rather than abort the baby leads to polarization between dads and moms. Many dads are like, “No, don’t do this, let’s end the pregnancy now.” And the mom says, “Well, wait a second. I’m not sick yet. I don’t want to give up yet.”
When I aborted those children right away, I would’ve said to the mother: “I saved your life.” But in our collection of thirteen, fourteen cases at Tepeyac, they all made it. And I’m just interested in accompanying people through really tough illness and disease without pitting the mom against the baby.
When young pregnant women come to the office and are considering abortion I say, “I’ve done that. I used to do abortions in this case, but I don’t anymore.” And I tell them: “You can go elsewhere. I can’t help you do that, but you can always come back to me for any complications. Why? Because I value you. I value your decision even though I don’t do it. You’re always welcome with us.” And you’re trying to meet them in their shame, in their pain which often tells them that they have no choice and that they have to get an abortion: “I have no choice. I have to do this.”
LS: I want to ask you about that open door. Your story isn’t simply as a story about walking away from abortions. You didn’t just give something up, you deliberately took on something new.
You talk about having a particular call from Mary to “always see the poor and see them daily.” That’s very different from just saying “I won’t perform abortions anymore.” It changed where you could practice as much as not doing abortions did. Can you talk about what that changed for you as a doctor beyond just, “I won’t do abortions”? How did that change where you and how you could practice?
It’s very rewarding to practice excellent women’s health that is collaborative, integrated, holistic, and listens to their bodies.
JB: When I was in undergrad and in medical school, I went and worked in Appalachia. But [students in medical school often] want to go on mission trips. Well, with all due respect, just look in your own community. There are men and women who live right next to you who are living below any level of dignity.
People like Paul Farmer from Harvard working in Haiti show that health is based on relationships. Medicine is an act of mercy. Again, you hate the disease, but love the patient. By collaborating in community, you can build a space where abortion becomes unwanted and children welcomed.
It’s very rewarding to practice excellent women’s health that is collaborative, integrated, holistic, and listens to their bodies. Children are not STDs. Fertility is something to be collaborated with rather than suppressed.
LS: I wanted to ask about the practicalities of living out that commitment. When a woman walks in your door who’s vulnerable, how big is the gap between the care she needs and the money available for it?
JB: Huge.
LS: Just ballparking, what percent is able to be paid for, and what percent has to come from donors?
JB: We were a for-profit medical practice. And all my bean-counter accountants were saying, “You got to stop seeing the poor.” Well, I couldn’t because that’s obedience. I believe in alms-giving because it’s very connected to medicine as mercy.
So practically, we probably raise 40 to 50 percent of the cost of our care. People sometimes ask, “Well, what was your plan, John?” I had no plan.
I have a budget now, but somehow I don’t think of it as seriously as my board does. I’m so grateful to my board for trying to keep us on the straight and narrow.
But I had dinner with Mother Angelica years ago. She was so excited about what we did before she died. She said, “Johnny, just remember, my son, budgets are for people who are fearful.” And I can tell you in my life, I’ve never been outdone in generosity. That weekend that we realized that our malpractice premiums tripled from a total of $80,000 to $240,000, and we had one month to cover it. A bunch of patients created an email list and we raised $242,000 in a weekend. It’s about having so much street credibility that you can go to your patients and beg.
LS: Let me ask you one last question. This is for someone who may be starting medical school who has a strong pro-life commitment, but wants to avoid the coarsening effect of medical school. They want to avoid that sense of becoming a vending machine that does procedures, not a person in relation with the patient.
What should this person take on outside of school as a counter-formation to the conventional formation of medical school?
JB: Two things: keep up your prayer life, that quiet time, however you do that. The second piece is to reach out to places like us at divinemercycare.org who can then connect you with Christian Medical and Dental, Catholic Medical Association, where you realize you’re not alone.
I was at the University of Virginia twelve years ago, a fourth-year resident walks up to me after my talk, during which I had asked: “If abortion is so good, why don’t more of us do it?” He comes up and says, “Do you really believe, Dr. Bruchalski, that life begins at fertilization, human life?” I said: “Oh, yeah. And it deserves our care.” He goes, “You’re the first person in twelve years of my academic training ever to have said that.” He said, “I find it fascinating.”
Transforming hearts through healthcare comes by one-on-one.
LS: Thank you so much for making the time to talk to me today. Dr. John Bruchalski, the author of Two Patients: My Conversion from Abortion to Life-Affirming Medicine. Thank you so much for your time.
By Daniel Sokol.
When not working as a barrister, I teach medical ethics to doctors who are going through disciplinary proceedings. The majority are in trouble because of dishonest conduct. They may have lied on a job application, cheated in a membership exam, or forged a document for personal gain.
Medical Practitioners Tribunals have often noted the difficulty of remediating dishonesty. If a doctor harms a patient because they cannot put in a central line safely, then a practical course on this clinical skill should remedy the problem. But what is the equivalent intervention if the failure is not a demonstrable skill but a character flaw?
My goal was to find a way of helping doctors show their knowledge and understanding of honesty.
I discovered that some employers used ‘integrity tests’ to screen suitable candidates. However, these tests were focused on selecting productive and dependable employees and were of limited application to doctors. Personality tests, like the HEXACO Personality Inventory, were too broad in scope, assessing honesty but also emotionality, agreeableness and conscientiousness.
Following discussions with a number of testing experts, it was decided that a situational judgement test (“SJT”) that encompassed a range of clinical and non-clinical scenarios would be best.
I worked with Rob Williams, a Chartered Psychologist with over 25 years’ experience of designing tests. He recommended producing scenarios which asked respondents for their best and worst answers, with each correct answer scoring one mark.
I compiled 31 scenarios from a mix of my own cases and published cases of the Medical Practitioners Tribunal Service (“MPTS”). It was important, I felt, for the scenarios to be based on actual cases to avoid the criticism of a lack of realism.
Initially, doctors were asked what they would do if faced with the scenario. The feedback from my erstwhile PhD supervisor, Raanan Gillon, was that this would unfairly penalise those doctors who answered honestly. Rob Williams agreed.
Doctors are therefore asked what they believe is the best and worst answer. Although there is no guarantee that the respondents would act honestly in these scenarios, the test at least shows their capacity to distinguish right from wrong in the domain of truth-telling and honesty.
The SJTs were then sent to Simon Fanshawe, a Diversity, Equity and Inclusion consultant, to check for bias and other impropriety in the scenarios.
Next, the SJTs were tested on 12 doctors, who were not told that this was an honesty test. A modest payment was offered to each volunteer. After this exercise, the number of scenarios was reduced to 23. The dominant reason for removal of a scenario was that the circumstances were too unfamiliar for the average doctor. The second reason was excessive variation in the answers selected. Below is an example of a discarded scenario:
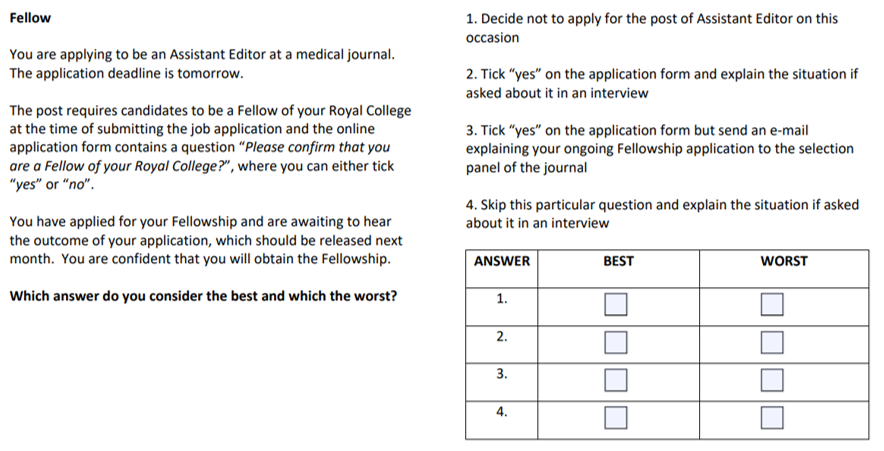
After the testing phase, I contacted the MPTS to ask if tribunal members could be approached to take the test. Their anonymous answers would represent what is “right” and “wrong”. The MPTS was reluctant and so I turned to UK-based professors of medical ethics who are also medical doctors. The medical requirement greatly limited the number of eligible respondents but it was necessary to avoid the likely criticism that the experts were unfamiliar with the realities of clinical practice and life as a doctor. A sum of £100 was offered for their participation. Six professors took part. Again, I did not present this as a test of honesty but described it as a tool to be used in the ethical training of doctors.
As a result of the professorial feedback, one scenario on practising medicine without insurance was removed. It was deemed of limited relevance to doctors without a private practice. The scenario appears below:
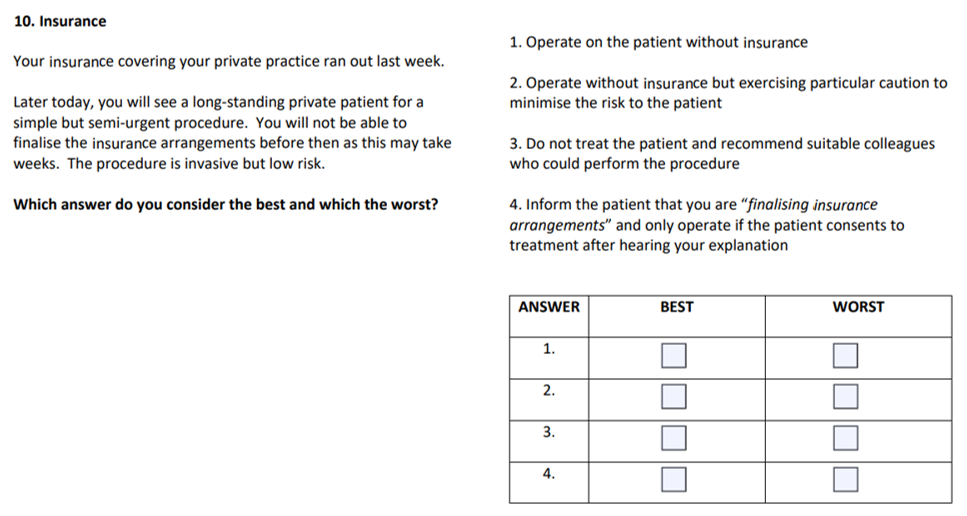
In the remaining scenarios, there was unanimous agreement in 32 answers and, for the remaining 12 answers, 5 out of 6 experts selected the same responses.
To the best of my knowledge, this test is the first honesty test for doctors. It cost approximately £4,300 to create, excluding my time and that of my assistant. It was funded privately. Everyone who has seen a version of the test has been asked to maintain strict confidentiality. Only my assistant and I know the collective answers of the Professors of Medical Ethics. To minimise the risk of a leak, the test is only administered in person.
At the end of the ethics training, I invite the doctors to complete the test. This takes approximately 25 minutes. Afterwards, we discuss each scenario, spending more time on those which the doctor found trickier.
Once they have completed the test, I invite the doctors to create their own scenario, based on their circumstances. This encourages them to think critically, and from a different vantage point, about their case. This genial idea came from Raanan Gillon, who told me that medical students at Imperial College had been asked to conduct a similar exercise in their ethics exams.
The feedback by doctors has so far been positive, with several observing that they had encountered some of the scenarios in their practice.
Recently, I approached a commercial research organisation to administer the test to 300 UK-based doctors. This would establish an average score, against which an individual doctor’s performance could be measured. However, as the proposed cost was close to £42,000, I was unable to implement this stage. It would be fascinating to administer the test to a large number of doctors and, indeed, members of the public. How would the scores of doctors undergoing disciplinary proceedings differ, if at all, from other doctors? Would doctors score higher in the test than members of the public? Would there be variations in test scores within the medical profession and, if so, why? It is an area ripe for empirical research.
Author: Daniel Sokol
Affiliations: 12 King’s Bench Walk Chambers, London, UK; medical ethicist
Competing interests: Daniel Sokol is the creator of the Situational Judgement Test
Social media account of post author: @DanielSokol9; Website
The post Developing an honesty test for doctors appeared first on Journal of Medical Ethics blog.
By J. Y. Lee.
Over the past week, a flurry of articles on the internet (for example: 1, 2, 3) sensationalized the contents of a journal article published by philosopher Anna Smadjor, on what she calls “Whole body gestational donation” – with discussants on social media largely condemning the proposed concept, and implying that “bioethics” itself is a corrupt field rife with repugnant ideas.
Smajdor’s work builds upon on an earlier paper by Rosalie Ber, who suggested that one way to avoid moral issues raised by gestational surrogacy might be to use female patients in a persistent vegetative state (PVS) – who had given prior consent – as surrogates. While Ber did not articulate a term for this concept, Anna Smajdor names this idea whole body gestational donation (WBGD).
Smajdor points out, quite plausibly, that just as some people would be prepared to donate parts of their bodies for organ donation, some may also plausibly be prepared to donate their whole bodies for gestational purposes. She suggests that states and health services – wherever organ donation is legal – might adapt their policies so as to allow for WBGD, as one option among other organ donation options. This means that people, just as they may elect and consent to donate some of their organs in case of their eventual death, might likewise consent to donate their whole bodies for gestational purposes in advance – or so her claim goes. On this framework, WBGD could theoretically be enacted in eligible brain-stem dead patients. WBGD would of course be “qualitatively different in that entails ventilation over an extended period,” in addition to the fact that it is not life-saving in the way people often understand organ donation to be. Rather, WBGD is proposed as a potential way to benefit aspiring mothers (or parents) who wish to avoid the risks and burdens of gestating with their own bodies.
Make no mistake – many ethical issues warrant continued discussion in this case. Smajdor fully acknowledges that “prolonging ventilation and somatic survival in brain-dead patients is undoubtedly a disturbing prospect,” given that WGBD would make salient the way a patient’s body can be completely instrumentalized for other people’s benefit. However, she believes – rightly so – that many of the ethical concerns which might follow WBGD have a similar structure to the concerns raised for other areas of reproductive medicine and organ donation. Thus, the fact that WBGD is riddled with various (though, in the end, standard) ethical concerns – like many other areas of medical practice – is obviously not itself a reason to shy away from raising the idea.
While I make no comment as to whether WBGD is a good idea overall, or whether it is something that I believe people in general might (or should) somehow come to accept morally, much of the reaction to Smajdor’s work, and the accompanying reaction to bioethics as a field, strikes me as misconstrued. One online article claims that “the body, even in death, still demands respect, and Smajdor’s proposal is not only disrespectful, but also dehumanizing and exploitative.” These are certainly ongoing concerns echoed in both the realms of organ donation as well as surrogacy, where ongoing bioethical debate offer rationales from different sides. Yet debates about what is or isn’t dignified, respect-worthy, exploitative, and so forth, are by no means settled. Smajdor’s justificatory scheme for WBGD is no different to the justificatory schemes that might be used in support of allowing commercial surrogacy, for instance. I myself have written critically about the objectionable ways that people overtly moralize commercial surrogacy (and in an accompanying JME blog post).
In fact, I can think of many other hard ethical cases up for debate which have not seemed to stir up the same condemnatory responses online. For example, many women with AUFI (absolute uterine factor infertility) find it acceptable to gestate their own child by receiving a uterus donation from living relatives (like one’s mother, aunt, or sister) or unrelated strangers willing to give up their uterus. This is despite the fact that a uterus transplant is not a ‘life-saving’ organ transplant, despite medical risks to both donor and recipient being widely acknowledged, and in spite of adoption and surrogacy being possible alternatives. The moral consensus when it comes to uterus transplantation, however, seems to be one of general excitement and continued endeavours to innovate. This is evidenced by the fact that, since the world’s first live birth via uterus transplantation in Gothenburg (Sweden) in 2014, research teams around the world have followed in Sweden’s footsteps. In the past couple years alone, many new countries have sought approval over their own uterus transplantation clinical trials – for example, in Australia and Japan. News headlines on this topic suggest that uterus transplants are ‘an amazing gift’, a stark contrast to the reaction borne by Smajdor’s suggestion to make it possible for people to donate their whole bodies for gestational purposes, despite there being clear parallels in terms of potential ethical worries.
While I am not suggesting that uterus donation is morally equivalent to whole body gestational donation, plausibly we might recognize that similar ethical concerns apply in both cases: we can question the conditions under which consent to be a donor/recipient for such a procedure might be legitimately given, we might anticipate the serious harms that might befall either party, contemplate the potential for emotional coercion and exploitation, and so on and so forth. Is it really, on balance, morally better to allow living uterus donors to undertake a risky, medically non-necessary, and non-life-saving procedure for people who wish to gestate, than to allow people to donate their bodies for gestational purposes in the event of their brain stem death? Of course, we might in the end find that the standard conditions proposed for uterus donation turns out to be more ethically acceptable on the whole relative to WBGD. But even if this were the case, such a result still does not speak in favour of taking the view that WBGD is a uniquely abhorrent or reprehensible proposal.
To point out another example, an article written by Didde B. Andersen in 2021 on vital organ donation makes a philosophical case for a radically permissive type of organ donation. Andersen argues that people – even people who are not imminently dying for other reasons – ought to be permitted to become living, vital organ donors. She says this may be permissible even when the donor risks incurring “non-trivial and irreversible harm (as is the case when he or she is not about to die for other reasons),” focusing on scenarios where the potential donors may voluntarily and autonomously wish to sacrifice themselves for others.
She calls this concept living vital organ donation (LVOD). Andersen’s LVOD is, in many ways, much more radical than Smajdor’s WBGD; for one, in the case of LVOD we are talking about patients who would still be alive at the time of donation but who would be killed in the process of the sacrifice. I think what the existence of this literature shows, however, is that bioethics, while it may sometimes be a platform for ideas we personally find repugnant, indeed remains an important field precisely because it is poised to debate a range of ethically difficult and complex matters. While some of these topics – and the mere fact of them put up for discussion in the first place – may strike many as completely alien to individual moral sensibility or gut instinct, it seems entirely reasonable, as well as valuable, for us to continue talking about issues for which people’s autonomy and welfare are at stake, and to reflect on why exactly we ought to approve or disapprove morally of both ongoing and prospective medical practices.
Author: J. Y. Lee
Affiliations: University of Copenhagen
Competing interests: None declared
Social media accounts of post author:
Twitter – https://twitter.com/jyleephilosophy
Webpage – https://www.jyleephilosophy.com
The post What’s the big deal with ‘whole body gestational donation’? On defending bioethics appeared first on Journal of Medical Ethics blog.