Is a 15-week limit on abortion an acceptable compromise?
A recent opinion piece by George F. Will, “Ambivalent about abortion, the American middle begins to find its voice” in the Washington Post made the startling claim that the overturning of Roe v. Wade (Dobbs v. Jackson Women’s Health Organization, 2022) has resulted in “a partial healing of the nation’s civic culture.” One might think exactly the reverse. The Dobbs decision energized voters, especially women and young people, resulting in numerous Republican electoral defeats across the country. However, Will argues that the return of abortion policy to the states gives voters the opportunity of choosing moderate restrictions on abortion. Since most Americans support early abortion while opposing late-gestation abortion, Will thinks that a 15-week ban on abortion would be an acceptable compromise.
Why 15 weeks? Two reasons can be given. Almost all abortions in the US—93%—occur within the first 15 weeks of pregnancy. For this reason, making abortion illegal after 15 weeks would not, it would seem, impose serious burdens on most people seeking abortions.
Another reason is that several European countries limit abortion on request to the first trimester, leading some US lawmakers to suggest that a 15-week ban would bring our abortion law in line with theirs. This is disingenuous, to say the least. While elective abortion is limited in some European countries, it is not banned afterwards, but is allowed on other grounds, including economic or social reasons, or a threat to the woman’s physical or mental health. Moreover, in most European countries, patients do not have to pay for abortion; it is covered under universal health coverage. The fact is that the trend in Europe has not been to limit abortion, but to expand access to it. Countries in Europe “… have removed bans, increased abortion’s legality and taken steps to ensure laws and policies on abortion are guided by public health evidence and clinical best practices.”
Were states to guarantee access to abortion prior to 15 weeks, a 15-week ban might be acceptable. However, even before Dobbs, many women in the US lacked access to abortion, due to a dearth of providers, especially in rural areas. They often had to travel many miles to find an abortion clinic, which meant that they had to arrange childcare if they have other children or take time off work. Delay is also caused by the need to raise money for an abortion, which is not paid for by Medicaid in most states, except in cases of rape, incest, or a life-threatening condition. To be sure, even if there were none of these roadblocks, some women would still not be able to have early abortions because they do not know that they are pregnant, due to youth, being menopausal, chronic obesity, or a lack of pregnancy symptoms. Any time limits will pose hardships for some people. But if access to early abortions were guaranteed, a compromise on a 15-week limit might be worth it.
I suspect that time-limit advocates are not particularly interested in making sure that women who have abortions get them early in pregnancy. They want to place roadblocks in the way of getting abortions, full stop. That these roadblocks increase the numbers of late abortions is of little concern to them, however much they wring their hands over late abortions. Abortion can be reduced by reducing the number of unwanted pregnancies, something that has been shown to be achieved by access to contraceptives and science-based sex education in the schools. Remember when pro-lifers emphasized those methods? Me neither.
“Some US lawmakers suggest that a 15-week ban would bring our abortion law in line with European countries. This is disingenuous, to say the least.”
My second concern is with abortions sought after 15 weeks. The reason for a late abortion may be that the woman has a medical condition that has not developed, or has not been detected, until later in pregnancy. In such cases, the pregnancy is almost always a wanted pregnancy, and the decision to terminate imposes a tragic choice.
It may be responded that all states allow abortions to be performed when this is necessary to save the pregnant woman’s life, and many allow for abortions to protect her from a serious health risk. The problem is that these exceptions conflict with standard medical care, especially in the case of miscarriage. Once the woman has begun to miscarry, the failure to remove the fetus is likely to cause her sepsis, which can be life-threatening. However, in states with restrictive abortion laws, doctors cannot perform an immediate abortion, which is the standard of care in such situations. They have to wait until her death is imminent and, in some states, they cannot remove the fetus until its heart stops.
Ireland’s restrictive abortion law was repealed after a woman who was denied an abortion during a miscarriage died from septicemia. To the best of my knowledge, no woman in the US has died as a result of restrictive abortion laws, but some have come close. An OB-GYN in San Antonio had to wait until the fetal heartbeat stopped to treat a miscarrying patient who developed a dangerous womb infection. The delay caused complications which required her to have surgery, lose multiple liters of blood, and be put on a breathing machine. Texas law essentially requires doctors to commit malpractice.
Conservatives often portray those in the pro-choice camp as advocating abortion until the day of delivery, for trivial reasons. This is deeply unfair. If they want us to compromise on time limits, they should be willing to guarantee access to abortion before 15 weeks. They should be willing to compromise on pregnancy prevention through contraception and sex education. And they should agree to drop all restrictions on late-term abortions that make legislators, rather than doctors, in charge of deciding what is appropriate medical care for their patients.
Featured image: Gayatri Malhotra via Unsplash (public domain)
Evangelium Vitae: the gospel of life. What is that gospel—that good news?
It is the good news—the very good news—that each and every member of the human family, as a creature fashioned in the image and likeness of the divine Creator and Ruler of all, is the bearer of profound, inherent, and equal dignity.
It is the astonishing news that, in the human family, everyone’s life is inestimably precious; there are no inferiors and no superiors in essential worth and basic rights.
It is, of course, true that people are different and, indeed, unequal in myriad ways. People are far from alike or equal in strength, intelligence, beauty, skill, dexterity, deftness, wit, and charm, as well as in wealth, power, influence, and social status. But the gospel of life relativizes all those differences and inequalities.
As creatures made in the image and likeness of God, every member of the human family is entitled to be treated with dignity and have his or her fundamental rights—beginning with the most fundamental and foundational of all rights, the right to life—honored, irrespective of such things as race, sex, and ethnicity, to be sure, but also irrespective of age, size, location, stage of development, or condition of dependence.
As children of the common Father, in whose image we are made, we human beings are a family. We are quite literally, and not merely metaphorically, brothers and sisters. Our bonds are familial bonds; our obligations to each other, familial obligations.
Injustices—above all, the unjust taking of human life—are not and can never be “none of our business,” for we are, again literally and not merely metaphorically, “our brother’s keeper.” And so our obligations—and let me be clear, our duties as a matter of justice to others—are not confined to not unjustly taking life. They extend to protecting others from those who would unjustly take their lives. When we fail in those duties, we commit injustices against those to whom the duties are owed.
Today, in the case of the precious child in the womb, justice demands not only that we refrain from taking his or her life, or directly cooperating in his or her destruction; justice requires that we, especially in our role as citizens, protect our unborn brothers and sisters and resist those who would expose them to the lethal violence of abortion. It is our fundamental duty in justice to demand that they—and everyone else—be afforded the full and equal protection of the laws. Those holding public office and exercising political power who sin against unborn babies, by exposing them to violent attack, commit a grave injustice. This injustice is intensified, not mitigated, when they claim to be people of faith and rationalize their wrongdoing by averring that they are simply declining to impose their religious beliefs on others.
Justice requires that we, especially in our role as citizens, protect our unborn brothers and sisters and resist those who would expose them to the lethal violence of abortion.
The very same principles require that we reach out in love and compassion to the precious mothers of unborn children—mothers who sometimes are indeed in gravely difficult, dangerous, even dire situations; mothers who are often under intense pressure from boyfriends, husbands, parents or other relatives, or employers—intense pressure to, in those shockingly callous but all too familiar words, “get rid of it.” Our motto—“Love them both”—is more than a slogan. It is more than a pledge. It is not something “beyond the call of duty.” It is our duty. And it is a duty that the pro-life movement, contrary to the vile slanders of the pro-abortion movement and the chorus that echoes its talking points in the media, has been fulfilling for the more than five decades of its existence.
Can our movement do still more? Should we do more? Yes and yes. We can. We should. And we will. What we will never do is offer our beloved sisters the ghoulish pseudo-compassion of the abortionist’s knife. We will offer, instead, the healing balm of genuine compassion, compassion born of love, compassion that offers, not a quick and easy, but deadly, “solution,” but rather an open-ended, open-hearted, self-sacrificial commitment. We have done this for fifty years. We will continue to do it.
What we will never do is offer our beloved sisters the ghoulish pseudo-compassion of the abortionist’s knife.
The Pro-Life Movement, before and after Roe
My own mother recruited me into the pro-life movement when I was a young teenager. This was before the Supreme Court’s decision in Roe v. Wade. Our movement formed in response to legislative efforts to weaken the protection of unborn children in states like Colorado, California, and New York. Those efforts were the work of a new movement that viewed abortion as the solution to two types of problems, the personal problems of women whose pregnancies were undesired and unwelcome, and the social problem of poor—and let’s not hide this fact—often minority children being born, children who, the pro-abortion movement said, would end up on the welfare rolls at taxpayer expense. The pro-abortion movement was further animated by the liberationist ethic, especially the sexual liberationist ethic, of the 1960s, and the belief—a ridiculous belief, as it turned out, but one widely held by elites at the time—that a so-called “population bomb” was on the verge of creating massive worldwide famines in which hundreds of millions, perhaps even billions, of people would die.
The pro-abortion movement claimed, knowingly falsely, that abortion needed to be legalized because tens of thousands of women each year in the United States were dying as a result of illegal, so-called “back alley” abortions. I repeat, and emphasize, that the pro-abortion movement made this claim while knowing it was false. We know that they knew, because the late Dr. Bernard Nathanson, a founder and leader of the movement, and himself a prominent abortionist, later in his life embraced the pro-life cause and revealed to the public that he and his colleagues knew the claims they made about death rates from illegal abortions were untrue—indeed, wildly untrue—when they made them. Nathanson also revealed that the movement he helped to found and lead, deliberately appealed to and stoked anti-Catholic prejudice to advance their cause, portraying opposition to abortion as nothing more than a reflection of Catholic dogma, and making the Catholic Church and faithful Catholic people out to be villains, who would rob others of their basic liberties, by imposing on them with the force of law their essentially sectarian religious precepts.
On the afternoon of Monday, January 22, 1973, I finished classes in the early afternoon and drove across town from my high school to join some women from my mother’s pro-life group in working a table at the West Virginia University student center, known as the Mountain Lair. As we were handing out our literature, a student walking past our table said to us, “Hey, there’s been a big decision from the Supreme Court on your issue.” “What is it?” we anxiously asked. “I don’t know” he said, “but it’s been on the news.” Well, we scurried off to find a radio—there being no internet or quick source of breaking news in those days. Then we waited for the hour, because there were no all-news channels; news was delivered “every hour on the hour.” We held out the hope that perhaps it was a big pro-life victory. But it was, of course, the very reverse of that. A constitutional atrocity and a moral catastrophe: Roe v. Wade.
To say that we were stunned would be the understatement of the century. After all, even non-lawyers knew that there was nothing in the text, logic, structure, or historical understanding of the Constitution that could provide a basis for the Court to declare a right to abortion, much less the sweeping right that was proclaimed in Roe v. Wade. It was clearly an illegitimate decision—in the words of dissenting Justice Byron White, an “exercise of raw judicial power.” On that day, our little group in West Virginia, like pro-lifers all across the country, vowed: “This will not stand.” We committed ourselves—our lives—to the project of overturning Roe. We didn’t know if it would be a five-year project, a ten-year project, or a twenty-year project. None of us, I suspect, thought that it would be a project that would take forty-nine years, five months, and two days. But we were determined to work as hard as we could for as long as it would take, even knowing that success in overturning Roe would only enable us to begin the next project—working through the mechanisms prescribed by the Constitution to secure for children in the womb actual legal protections, a project that would require us to persuade our fellow citizens to fulfill America’s promise of liberty and justice for all by bringing the unborn under the mantle of the law’s protection.
On that day, our little group in West Virginia, like pro-lifers all across the country, vowed: “This will not stand.” We committed ourselves—our lives—to the project of overturning Roe.
That, of course, is the challenge we face today. It is a challenge made even more difficult by the nearly fifty-year reign of Roe v. Wade. That is because, as Aristotle observed long ago, the law is, among other things, a teacher, a giver of moral instruction, a former of consciences. For forty-nine years, five months, and two days, our law taught a gross moral untruth. It taught generations of our people that the choice to destroy a child in utero is a basic liberty—indeed, a fundamental right. It taught that that the child himself or herself is as nothing—a blob of tissue, a meaningless mass, a mere object, a piece of property, rather than a person with dignity and a right to life. That is a false lesson that it is our job to help people to unlearn. And that will take effort … and time. We will, as Ryan Anderson, who leads the Ethics and Public Policy Center in Washington, D.C., has recently pointed out in an excellent Wall Street Journal essay, need to go step by step, moving forward with determination and with prudence toward our goal of an America where every child is protected by law and welcomed in life. Victory will not come all at once, but each legislative achievement will plant the seeds of the next one.
A Dozen Pro-Life Heroes
I’m keenly aware that this is the first awarding of the Evangelium Vitae medal since the overturning of Roe v. Wade—an achievement that many people, those sympathetic to our cause as well as those unsympathetic to it, thought was not possible. After all, our opponents had everything going for them: power, money, prestige, control of the leading institutions of education, culture, philanthropy, entertainment, the economy, and, of course, the news media. We had, and have, none of those things. And yet, the reversal of Roe was made possible because pro-life people all over the country, people like my mother, never lost faith, never gave themselves permission to give up. Even in the face of devastating disappointments and betrayals, such as the grievous 1992 decision of the Supreme Court in Planned Parenthood v. Casey, they kept hope alive and soldiered on.
It is on their behalf that I accept the Evangelium Vitae medal. I am not worthy of such recognition. They are. And I would like this evening to mention just a few heroes of our movement who did not live to see Roe fall, though they worked their hearts out to bring down that dishonorable decision. I hope that you will always regard them as the true recipients of the 2023 Evangelium Vitae medal. A complete list would include many more names than I will be able to mention and briefly profile. By no means am I diminishing the contributions of heroes I do not mention. But I would like to say a word about some of my personal pro-life heroes, people I knew and in some cases had the privilege of working closely with.
Dr. Mildred Jefferson was the first black woman to graduate from Harvard Medical School and the first woman to graduate in surgery from Harvard. She worked tirelessly to defend unborn babies and, after Roe was handed down, to overturn it. She was an implacable foe of the dehumanization of anyone, anywhere. She served three times as President of the National Right to Life Committee. She was my friend. I drew inspiration from her.
Congressman Henry Hyde labored tirelessly, year in and year out, to protect unborn babies and overturn Roe. He was our champion in the fight to ensure that taxpayer dollars were not used by the federal government to fund elective abortions. He too was my friend, and I had the honor of working with him on many occasions.
Mrs. Nellie Gray was the indomitable, unstoppable founder and leader of the annual March for Life. It is simply impossible to exaggerate the role of the March, and thus the importance of Nellie’s work, in keeping the flame of hope burning in the pro-life movement. Nellie was the living embodiment of our movement’s determination to prevail, no matter the cost, no matter the sacrifices, no matter how long it took. The March was for Nellie quite literally a labor of love. And she taught all of us in the movement to see our work in precisely that way. Love for babies. Love for mothers. Love as the answer to the violence of abortion.
Fr. Richard John Neuhaus was a mentor and one of my dearest friends in the world. As a young Lutheran pastor, he had been a leader in the anti–Vietnam War movement and in the civil rights movement, where he marched literally arm-in-arm with Rev. Martin Luther King. A gifted thinker and a brilliant speaker and writer, he was poised to become America’s next great religious public intellectual, the successor to Reinhold Niebuhr. But then the liberal establishment opted, tragically, to embrace abortion. Pastor Neuhaus had to choose whether to make himself acceptable to the cultural, educational, and economic elite—an elite that would, if he yielded on the question of abortion, confer upon him the highest forms of status, recognition, and worldly honors—or stand with unborn babies and their mothers. For Neuhaus, it was an easy choice, and required not even a moment’s deliberation. He became our movement’s intellectual and, in many ways, its spiritual leader. His vow, that we will “never weary, never rest” until all our nation’s children are protected in law and welcomed in life, became our rallying cry.
Governor Robert P. Casey, the last of the great pro-life Democrats, was one of the most principled men I ever had the honor to know. I had the privilege of working with him as an advisor and speechwriter on pro-life issues. When he was told, by no less than James Carville, who was running his campaign for Governor of Pennsylvania in 1986, that unless he “softened” his opposition to abortion he would lose, he simply responded, “then I will lose.” He won. Then, after pushing major pro-life legislation through the Pennsylvania legislature, he won again in 1990—this time over a pro-abortion Republican opponent and by a landslide of historic proportions. Governor Casey showed other pro-life politicians that leaders lead, and that by proclaiming and defending pro-life principles, pro-life candidates can win elections despite polling suggesting that the pro-life position is a “political loser.” Pro-life politicians need to be reminded of that message today.
Notre Dame’s own Professor Charlie Rice was one of the intellectual architects and leaders of the pro-life movement. A Marine lieutenant colonel and a legal scholar, he taught generations of Notre Dame law students—and lots of us who were not formally his students—how to make the legal case against Roe and for the child in the womb. He brought together reason and passion in a way I found remarkable and inspiring. He knew how to be tough in making an argument without being a bully. That’s because he was genuinely devoted to the truth, and in that way was a truly exemplary scholar and teacher.
Mr. Joe Scheidler, whom I had the honor of meeting on one or two occasions, was an advertising executive who took our nonviolent movement to the streets in the way that Martin Luther King took the civil rights movement to the streets. The New York Times, an organ that is scarcely sympathetic to the pro-life cause, acknowledged Mr. Scheidler’s effectiveness, noting that he “became a leading figure in the anti-abortion movement by marrying media savvy with confrontational tactics.” That, indeed, he did. A graduate of Notre Dame, Scheidler was known not only for his willingness to be confrontational, but also for his ability to be in dialogue and even friendship with abortion advocates, such as Bill Baird. His pro-life convictions were born of love, a love so great that it would not only prompt him to bear enormous personal risks and make profound sacrifices on behalf of the babies, but also enable him to regard even his most determined adversaries as friends to be loved and cherished, not enemies to be hated and destroyed. For Mr. Scheidler, no one was beyond redemption.
Germain Gabriel Grisez was my intellectual godfather. His 1970 book Abortion: The Myths, the Realities, and the Arguments remains one of the greatest works of scholarship on the subject ever produced. Were the expression of truth by itself capable of resolving disputed questions, the debate over abortion would have ended in a grand pro-life victory three years before Roe v. Wade was decided. In our world, though, truth, even when stated plainly and defended decisively, can be obscured, or ignored, and shunted aside. Still, Grisez’s work enabled the pro-life movement to proceed with profound confidence in the intellectual integrity and soundness of its convictions—and this was no small thing. To this day, it is in many ways unsurpassed.
Mother Teresa of Calcutta, in 1994, literally petitioned the Supreme Court of the United States in an amicus curiae brief to “reverse Roe v. Wade and declare the unalienable right to life of the unborn child.” Due to the kindness of my friend, pro-life attorney Harold Cassidy, I had the honor to be Mother’s lawyer as lead counsel (what is known as “counsel of record”) on the brief—a brief whose principal draftsman was not me, but was rather my beloved friend William Porth, with whom I worked.
Dr. Hymie Gordon was a deeply observant Jew, the son of a rabbi in South Africa, who came to the United States to make his career in medicine, first at Johns Hopkins and then at the Mayo Clinic, where he established a pioneering program in medical genetics. Known as “the father of fetology,” Dr. Gordon was a profound believer in the sanctity of human life, and a physician and teacher who dedicated himself to the Hippocratic oath and the principles of Hippocratic medicine. He was appalled by the decision of medical school after medical school to remove from the oath its express prohibition on physicians inducing abortions. When medicine, as a profession, began heading down the wrong path, he spoke as a prophet—an Elijah, a Jeremiah—reminding his colleagues that the presence of a human being from conception forward was an established scientific fact, not a matter of metaphysical speculation or religious dogma, and calling out academic medicine for compromising its most basic values and abandoning its vocation to heal the sick and infirm and preserve human life.
John Cardinal O’Connor, the late Archbishop of New York, above all others, stood up to those politicians who, while professing to be “personally opposed” to abortion, supported its legal permission and even its public funding, ostensibly on the ground that to do otherwise would be to impose their religion on other people, in violation of the Constitution. This argument was absurd on its face, since the science of human embryogenesis and intrauterine development is clear, and unanimous, and has been for more than fifty years. It was never—I repeat, never—made in good faith, not by Mario Cuomo or Geraldine Ferraro in Cardinal O’Connor’s time, not by Joe Biden or Nancy Pelosi or anyone else today. At a time when many religious leaders, for whatever reasons, were unwilling to call these people out for their bad faith and manifest injustice toward the most defenseless and vulnerable members of the human community, Cardinal O’Connor publicly confronted them and held them to account.
Nat Hentoff (who, as it happens, wrote a splendid, appreciative biography of Cardinal O’Connor), was the jazz music critic for the Village Voice newspaper, as well as its leading writer on civil liberties. He was an atheist, an old-school liberal, and a longstanding member and board member of the ACLU. Initially, he was fully onboard with abortion “reform.” But then he learned about “Baby Doe,” an infant diagnosed with a cognitive disability who was left by the parents and hospital staff to die. Outraged, he made a national issue of the Baby Doe case, only to find that his fellow liberals were all for abandoning the baby. If abortion was okay, they reasoned, what could be wrong with the infanticide of an infant whose life allegedly “wasn’t worth living’”? My friend Nat was shocked and scandalized by their reaction, and it made him think. If infanticide is not okay, how can elective abortion be okay? A man of unflinching intellectual honesty and moral integrity, he suddenly found himself in a place he never imagined being. He was a convert to the pro-life cause, and a passionate defender of the lives of all children, especially those most vulnerable—the unborn and disabled newborns. He wore his excommunication from the ACLU—which came, as you can imagine, in short order—as a badge of honor.
The Battle Ahead
Well, there you are. A dozen pro-life heroes, twelve apostles of life—from the atheist liberal Nat Hentoff to the Catholic saint Mother Teresa of Calcutta. We in the pro-life movement owe each of them an enormous debt of gratitude and we can and should continue to draw inspiration and strength from their work and witness.
It will be hard. We will have moments of disappointment. We will experience setbacks and, alas, betrayals. But we will not lose heart.
And we will need that inspiration and strength, because, as I suggested a moment ago, now we face an even more daunting challenge than reversing Roe v. Wade. With Roe gone we are finally on the field of battle, but powerful forces are arrayed against us.
Nevertheless, “with malice towards none, with charity for all, with firmness in the right as God gives us to see the right, let us strive on to finish the work we are in.” It will be hard. We will have moments of disappointment. We will experience setbacks and, alas, betrayals. But we will not lose heart. We will not lose faith. We will not abandon hope. For we know that “He has sounded forth the trumpet that shall never call retreat. He is sifting out the hearts of men before his judgment seat. Oh, be swift my soul to answer him, be jubilant my feet, for God is marching on!” And under His hand of blessing, trusting that He will never leave unaided those who in a righteous cause call upon His help, we shall overcome.
These remarks were delivered at the University of Notre Dame’s de Nicola Center for Ethics and Culture on April 29, 2023.
![]()
Gov. Ron DeSantis of Florida at a bill-signing event this month.
![]()
![]()
![]()
By Anthony McCarthy
Some women regret their abortions. Does this tell us anything interesting about whether abortion is, morally or prudentially, a choice worth making?
A number of empirical papers have assessed the prevalence of abortion regret, reporting that a large majority of women do not regret their abortions. While use of the Turnaway Study data set has been subjected to some critique, not least because of the high dropout rate, these papers have undoubtedly received huge media coverage. Much less well-covered is a study by some of the same researchers using the same data set which found that 96 per cent of women who were refused abortions did not regret having the child 5 years on.
One serious attempt to deal with the subject of abortion regret in terms of moral philosophy is Kate Greasley’s ground-breaking 2012 paper in the Journal of Medical Ethics, to which I recently responded in Theoretical Medicine and Bioethics. Greasley argues that regret over abortion decisions does not neatly track moral and rational justification. She suggests that any discrepancy there may possibly be between regret for abortion and for giving birth can be readily explained by the ‘affirmation dynamic’, an idea deriving from the philosopher RJ Wallace. Adopting this idea, Greasley explains that a pregnant woman will be subject to a parental duty to affirm the life of her child, which will preclude regret over her reproductive choice…there may have been serious objections to continuing the pregnancy. If this was the case, then such objections would continue to stand even if the girl chose to complete her pregnancy, thus finding herself in a position where she could not regret her choice…If the girl has her baby, we know that the non-availability of regret has nothing to do with justification. The presence of regret in the abortion scenario does not therefore take on justificatory significance simply because, had she kept the pregnancy, she would eventually have to affirm her decision.
Greasley argues that a woman who gives birth is morally obligated to love and value her child and therefore (Greasley thinks) is obligated not to regret a decision to have the child – she cannot regret a decision with an outcome she welcomes and should welcome. No such obligation exists for a woman not to regret her abortion.
In response to this, regretting a choice and regretting its outcome can be separated here as elsewhere. For example, can a woman not regret her abortion simply because it has resulted in a new child whom she loves and who would not have existed without the prior abortion? In the same way, a woman who conceived deliberately as a young teenager, a case discussed by Greasley, can reasonably love and welcome her child while still believing she was wrong to seek conception in less than adequate circumstances and morally regretting that she did so.
Moreover, simply because it may be psychologically difficult for a woman to regret having her baby does not mean her testimony should be set aside. Quite generally, if one group of people is, for reasons separate from the justification of a choice they made, less likely to have an opportunity to experience regret, this does not mean that any regret experienced by a contrast group is necessarily unreasonable, or that the possibility of such regret should not influence others’ decision-making.
Think of a group of soldiers who initially believe that use of ‘enhanced interrogation techniques’ is justified in certain circumstances where it can save lives by preventing acts of terrorism. If some are successful in saving lives this way, it may be harder for them to develop regrets – the success insulates them from such feelings – than it is for those who fail to extract information using the same techniques. But that does not mean that any regrets of the second group are irrelevant as evidence as to whether use of the techniques was morally justified. Such testimony can at least assist with discerning whether these techniques are right or wrong, even if those expressing regret are smaller in number than those who express no regret.
While regret is not morally infallible – justified actions can be regretted – regret for actions that end lives or otherwise cause serious harm should be listened to with particular care. And indeed, Greasley herself acknowledges that if at least “most people” experience regret at a decision to end a life, this is something that might “give one pause for thought.”
Greasley believes avoiding regret can be a reason to act or refrain from acting, even if regret’s “persuasive power only derives from the belief that regret will reflect justification”. However, post-abortion regret is not a mere feeling but relates to a value or values: the woman who regrets her abortion will likely regret ‘what she missed out on’ and/or ‘what her fetus missed out on’ due to the choice she made and this will (or may) reflect a rational judgement as she sees it. In contrast, a woman who goes on to have her baby – even after being denied an abortion – may regret aspects of her situation but is unlikely to regret having the child.
Even if most women do not regret their abortions, this does not deprive of justificatory moral significance, as Greasley appears to suggest (“regret has very little, if anything, to say about abortion’s moral or rational standing”), the reports of those who do regret their abortions. Nor does it deprive of justificatory moral significance reports of sadness, grief and guilt on the part of women who nonetheless deny regretting their abortions. In making a decision for herself, a pregnant woman who wants to avoid both regret (acknowledged or unacknowledged) and feelings of sadness, grief and guilt is justified in allowing the experience of women who undergo any of these reactions to inform her own decision.
Author: Anthony McCarthy
Affiliation: Bios Centre, London, UK
Competing interests: None declared.
Social media accounts:
https://twitter.com/BiosCentreUK
https://www.facebook.com/BiosCentreUK
The post Abortion and regret appeared first on Journal of Medical Ethics blog.
![]()
This article received an honourable mention in the graduate category of the 2023 National Oxford Uehiro Prize in Practical Ethics
Written by University of Manchester student Thomas Long
Abstract
This essay presents, first and foremost, the recollections of a doctoral anthropologist as they attempt to make sense of a moment of embodied, ethical dissonance: a moment where the “familiar” of their own ethical positionality was suddenly and violently made very “strange” to them through participation in applause. Applause is one of the most practical ways we can perform our support for a cause, idea or individual within corporeal social space. Through a vignette, I examine the ethical challenge presented by my own, unexpected applause – applause for the Pro-Life movement – that occurred during fieldwork with Evangelical Christians in the U.S.A. I use this vignette to question the impact of the field on an anthropologist’s capacity to practice what they see as good ethics, and in doing so, consider the practical ethical limits of conducting ethnographic research with so called “repugnant cultural others” (Harding 1991). I argue that moments of uncomfortable alienation from one’s own perceived ethical positionality present not a moral, but a conceptual challenge, in that through this alienation the elasticity of our ethical selves is laid bare. I conclude by suggesting that the challenge presented by doing ethnography with ethically divergent interlocutors constitutes an “object dissolving critique” (Robbins, 2003, p.193) of our implicit conception of what it means to be a coherent ethical subject at all.
About a month before the Supreme Court went public with its decision to overturn Roe VS Wade, the legislature protecting the right to an abortion in the U.S.A, the Southern Baptist Convention was holding its annual meeting in California. As the largest and arguably most politically conservative denomination of Evangelical Christians in the U.S, the SBC boasts a spanning network of cultural and institutional infrastructure, extending deep roots that perforate the fabric of society in the North-American South. At this year’s annual meeting – along with a scandalous report exposing an endemic sexual abuse problem within the denomination – Roe vs Wade and the burgeoning gains of a galvanised Pro-Life movement dominated centre stage.
Some weeks prior, a draft opinion document detailing the Supreme Court’s plans to overturn the historic constitutional amendment had been leaked to news outlet Politico, re-energising evangelical anti-abortion crusaders for whom an, albeit troubled, political intimacy with the Trump administration was continuing to bear fruit. For Southern Baptists, who – quite literally – consider abortion to be murder, this signified a great “victory for life” in what for over half a century had been widely considered a losing battle with death. There was talk of widespread elation and even parties being held amongst the Baptist community in celebration of the leaked opinion draft, and the excitement in the air at the annual meeting was palpable.
“Just imagine”, expressed an impassioned speaker presenting a panel discussion on the future of the Pro-Life movement in “a post Roe-V-Wade world”, “how many babies this will save if Roe is in fact overturned. How many of Gods children will be allowed a chance at life”. Discussing potential legislative options, another speaker described plans to lobby government “to treat the abortion pill like illegal contraband”, reminding the audience that half of all abortions are chemical abortions and likening the import of the morning-after pill to drug trafficking. A third gave a run-down of the Psalm 139 (V13-14: For you created my inmost being; you knit me together in my mother’s womb) project, an initiative with the goal of placing ultrasound machines in abortion clinics, in order to encourage potential mothers to “see their babies” before making the decision to terminate them. A smartly dressed attorney fiercely stated her pride at the readiness of Southern Baptists to “stand shoulder to shoulder in this fight for the dignity of women, the dignity of their children and the dignity of human life – God bless us all!”.
Having grown up in London and then moved to Manchester, bustling and politically liberal urban hubs where abortion remains a right and available for free on the NHS, this was the first time in my life that I had rubbed elbows with anti-abortionists, let alone hard-right “Christian nationalists”. Sitting there, engrossed and definitely a little shocked, I had my first encounter with the infamous political fervour that I had seen plastered all over newspapers and news stations since Trump’s election in 2016; The figure of the incandescent evangelical, inflamed by a fury and a fire conferred by God himself, draped, obtuse and unapologetic in red white and blue, and alive with a divine moral purpose that burned through the eyes and lashed off the tongue. Theirs was after all, a “moral majority”, an ideology powerfully infused and inseparable from an urgent ethical mission, to swim up the stream of a polluted and poisonous cultural swell, and save one nation-under-God from its own misguided modern circumstance.
It was, at once, everything that interested me about right wing Christian politics in the U.S, and everything that worried me about performing ethnographic research on it. With every new speaker, with every damning speech, and with every bout of growing applause for each, a paranoia was beginning to set in. I had begun to feel my presence as an ‘ideological outsider’ increasingly as the event went on, my sense of its perceived obviousness swelling like a balloon in the back of my head, giving me away to the rest of the room and to the big Other of the convention at large. I could say with some certainty that I disagreed quite strongly with almost everything the Baptists had to say, and the radical unfamiliarity of the lens through which they spoke about abortion had disturbed me in a visceral, discordant kind of way. This was that radical unfamiliarity distinctive of the ethnographic experience, in that it was as intrusive as it was intellectually invigorating. I could feel eyes upon me: lasers pointed at the back of my head that heated up my neck, to the point where I dared not turn lest the slightest movement somehow splinter and destroy whatever fragile façade of support I was still upholding, exposing me as an interloper to the entire room.
This was all, of course, completely in my mind. The Southern Baptists had been nothing but accommodating and friendly towards me the entire time I had been there, giving me a press pass, access to a break room and an unlimited supply of tea and coffee. They had welcomed me in as a university-based researcher knowing full well that I probably didn’t agree with their politics, and what’s more, I remember thinking that the idea someone was monitoring how I, a random observer in a sea of maybe four-hundred, was actively reacting to what was being said on stage, verged, quite frankly, on the schizophrenic. For whatever reason, this knowledge was powerless to relax me. I had expected when preparing for this project that my positionality would be challenged, that I would feel uncomfortable in the presence of “the repugnant cultural other” (Harding, 1991). I had not however, considered exactly what this would feel like in an embodied, practical sense. I had, in my naïve haste to intellectualise the field and my fieldwork, overlooked “the ethical as a modality of social action or of being in the world [more so] than as a modular component of society or mind” (Lambek, 2010, p.9); I had seen my own ethical positionality as something to be intellectualised also.
As the event came to a close, a final speaker expressed his gratitude for the other panellists, the audience, and for the work of the Pro-Life movement in general. “I just want to say that I am so, so proud to be a part of a community doing so much for life and for the unborn everywhere. We’ve had some great speakers tonight. Let’s now show our support for them, and their tireless work to make abortion not just illegal, but unnecessary and unthinkable! Amen people!”. The room erupted into thunderous applause, and it was only as the applause began to die down, that I realised that a pair of disembodied hands beneath my eyeline were applauding as well. The burning I had felt in the back of my neck remained but adopted new significance, as I realised that those hands – applauding a punitive ban on abortion – belonged to me. I felt guilt, shame, and inflaming both of these to the point where I broke out into a light sweat, a panicked sense of what I can best describe as alienation.
I had been in the field not three days, and felt as though I had already betrayed my own moral beliefs. I was, and remained, firmly pro-choice, not least because I felt my own gender disregarded me somewhat from any other kind of imposition. How on earth had I found myself in this situation, actively performing my support for a movement seeking to strip this choice from women? Applauding a ban on abortion? Really? When I had read in the past about “going native” – the moment in which “the anthropologist loses his supposed detachment, and throws over the world he was born into for the world he has found” (Wickham-Crowley, 2000, p.11) – I had never imagined this to be an exercise that would compromise my morality. I was not Pro-Life and was quite sure of this fact, so why did I feel so alienated from my own sense of morality?
The applause itself could be explained in a number of different ways. In an article about social production and shared ritual worship in Pentecostalism, for example, Joel Robbins (2009) uses Collins’ (2004) notion of “Interaction Ritual Chains” to explain the “emotional energy” (p.44) produced when acting as part of a group in a ritualised setting: a setting where a particular form of participation such as prayer – or indeed, applause (Remisiewicz & Rancew-Sikora, 2022, p.309) – is elicited as an aspect of an event’s sequence. Beginning from Durkheim’s (1995) argument “that major collective rituals produce a kind of effervescence that energizes people and leads them to feel empowered” (Robbins, 2009, p.60), Robbins suggests that the draw of shared participation in Pentecostal spaces lies less in their theology and more in their praxis: in their capacity for “emotional entrainment through bodily synchronization” (Ibid, p.61) that is difficult to resist and adept at interpolating the hesitant. It certainly seems a reasonable explanation to suggest that, given the affective power of the ritualised (and religious) emotional energy in the room – a powerful, politicised energy engendered by the Pro-Life movement’s envisioning of itself as a divinely commissioned “social crusade” to enhance women’s position (Ginsburg, 1998, p.218) – I had merely been swept up in an “Interaction Ritual Chain” of applause as it moved through the crowd. My participation was an arbitrary, physical response to stimuli rather than a practical ethical act in itself.
Also worth considering was the paranoid sense of otherness that I had felt so intensely preceding the moment of applause itself. Understanding the experience through a Foucauldian lens for example, renders the act less as an exposition of ethical subjectivity and more as the response to power of a disciplined body: “The body is also directly involved in a political field; power relations have an immediate hold upon it; they… force it to carry out tasks, to perform ceremonies, to emit signs” (1977, p.25). It could therefore be argued that applause here represented one such sign, its enactment engendered by my perceived “state of conscious and permanent visibility” (Ibid, p.201) located in the panoptic (Ibid) ideological gaze of some four-hundred Pro-Life advocates.
Both are sufficient explanations, and go some way as to explicating some of the practical ethical pressures that may be placed on an anthropologist during the ethnographic encounter. They do not, however, address the contradiction at the centre of my recollection: namely my guilt, panic and sense of moral alienation in light of the fact that I knew I was not Pro-Life. If I wasn’t feeling a sense of alienation from my own moral compass, then what exactly was I feeling? Perhaps the answer lies in the most basic and obviously disturbing element of the experience: that my surroundings had made my body act in a way my mind – and “heart” – did not condone. Perhaps what had disturbed me was the abrupt, practical demonstration of our environment’s power to alter our behaviour in immediate and unexpected ways, regardless of the moral ambiguity of that behaviour. And perhaps worse of all was the sense that I had been, in that moment, completely powerless to stop it.
As Lambek tells us, ethics often exists “in the movement or tension between the ostensible (manifest, explicit, conspicuous, declared, avowed, certain, normative, necessary) and the tacit (latent, implicit, ambiguous, subjunctive, aporetic, paradoxical, uncertain, transgressive, possible)” (Lambek, 2010, p.28). Bearing this in mind, the analytic potential of the ethnographic encounter for practical ethics thus becomes its ability to make poignantly visible the elasticity that this perpetual in-betweenness demands of the ethical subject. Being ostensibly pro-choice in an environment that demands (through interaction ritual chains or panoptic disciplinary power) a performance that is tacitly Pro-Life (namely, applause for the movement) indicates unequivocally a contradictory and elastic ethical self: an ethical self that is disembodied and impalpable enough to do both of these things simultaneously. It is here we find the locus of the alienation we have been seeking to root out.
In the sudden, dizzying realisation that the hands applauding one cause and the heart bound to another originate from the same subject, the formless contingency of the ethical subject is laid bare. At the absurd moment of this recognition, the illusion of our consistent ethical self is, for a brief moment, lost to us, and a sense of groundless, alienated dissonance creeps into our core. Not only does the field challenge our conceptual registers with radical forms of epistemological otherness and difference, it also pulls at the very substance of our ethical selves by situating them within an environment incongruent to their normative animation. Captured in my applause for the Pro-Life movement was thus not only a moment of moral slippage, nor a mere instance of participation in synchronised social activity. Neither can it be reduced to a simple concave to the (inferred) social pressure of my interlocutors. Instead, the event and its unsettling, introspective, alienating effect, represented a practical crystallisation of ethnography’s uncomfortable challenge to the ethical subject. The “object dissolving critique” (Robbins, 2003, p.193) of its own incoherence.
Reference List
Collins, R. 2004. Interaction Ritual Chains. Princeton, NJ: Princeton University Press.
Harding, S. 1991. Representing Fundamentalism: The Problem of the Repugnant Cultural Other, Social Research, vol. 58, no. 2, pp.373–93.
Durkheim, E. 1995. The Elementary Forms of the Religious Life. Trans. K. E. Fields. New York: Free Press.
Foucault, M. (ed.) 1977. Discipline and Punish: The Birth of the Prison. New York: Pantheon Books.
Ginsburg, F. (ed.) 1998. Contested Lives: The Abortion Debate in an American Community. University of California Press.
Lambek, M. (ed.) 2010. Introduction. In Ordinary Ethics: Anthropology, Language and Action, pp.1–36. New York: Fordham University Press.
Remisiewicz, Ł., & Rancew-Sikora, D. 2022. A study of applause in family ritual. Discourse Studies, 24(3), pp.307–329.
Robbins, J. 2003. ‘What is a Christian? Notes Toward an Anthropology of Christianity’, Religion, vol. 33, no. 3, pp.191–199.
Robbins, J. 2009. Pentecostal Networks and the Spirit of Globalisation: On the Social Productivity of Ritual Form. Social Analysis, Volume 53, Issue 1, pp.55–66. Berghahn Journals.
The Bible: New International Version, Psalm 139, Verse 13-14. Accessed 01.02.23: https://www.biblegateway.com/passage/?search=Psalm%20139&version=NIV
Wickham-Crowley, K. M. 2000. “Going Native”: Anthropological Lawman. Arthuriana, 10(2), pp.5–26. https://www.jstor.org/stable/27869541
![]()
Texas' multiple laws banning abortion have doctors speaking in code, refusing to counsel patients, and have essentially chilled their abilities to discuss abortion. Doctors are finding ways to suggest patients take a nice hike in a state that doesn't regulate women's rights to their own bodies, but even that seems risky. — Read the rest
![]()
![]()
In today’s interview, Leah Libresco Sargeant speaks to Dr. John Bruchalski. He is an OB/GYN based in Virginia, and the author of the recent memoir Two Patients: My Conversion from Abortion to Life-Affirming Medicine. Sargeant is the creator of Other Feminisms, a substack focused on the dignity of mutual dependence. Their conversation has been edited for length and clarity.
Leah Sargeant: Dr. John Bruchalski, you’re an OB/GYN who used to practice what people would think of as the full spectrum of obstetrics and gynecology, including abortion. And that’s something you chose to walk away from.
I want to ask you a little bit about that choice and about what your new practice looks like, starting with one of those pivotal moments you described in your book when you went into the operating room for an abortion and were confronted by a baby. Can you tell me about that night?
Dr. John Bruchalski: At that point, I’m working at a pregnancy center at night, but during the day, I am doing the full spectrum of OB/GYN, including aborting healthy children, sick children, just about for any reason at any time. Abortion on demand.
And that dissonance is becoming more and more tense for me.
So there I am in one room saving a 22-weeker because the mother desperately wanted it. She’s praying, she’s begging, she’s imploring. We have her in Trendelenberg [a position to forestall premature labor], kind of tilted backwards. We’re using medication and antibiotics, and she’s getting better.
In the other room, mom didn’t want it. She’s like, “No, just get rid of it.” And what did I do? I broke her water and pitted out the baby [administered Pitocin to induce labor].
Now the baby comes out and I lift it. And usually when a baby’s born alive in an abortion, we suffocate it [by not assisting breathing].
But it felt a little heavy. I threw the baby on the scale and lo and behold, 505 grams [over the legal limit, requiring life-saving treatment], I had to call the intensive care nursery. In walks Dr. Debbie Plum [from the NICU team], she takes one look and says, “Hey John, you’re better than this. Stop treating my patients as tumors.”
This baby weighed about a pound and a quarter. Its skin was translucent. It made noise, it was obviously human, part of our family. But the dissonance is: no, call it a fetus, it’s not wanted.
It’s unwanted. So therefore we need to terminate it. The mother doesn’t want it, society doesn’t want it.
LS: I was really moved reading your story of that night and that delivery. I went and looked up kind of what that critical threshold was for the baby. And it was five grams, you said, over the limit.
And so I looked up, what else is five grams? A sheet of paper. A sheet of paper weighs five grams. And that was the measure of what made someone a person or not in the hospital.
JB: That’s exactly right. Once you remove medicine from truth and justice and equality and equity and ecology, five grams—a sheet of paper or whatever the mom wants. It’s a desire.
I began to see my heart hardening as I was doing more and more abortions. You go from the little ones that have no bones to the ones that have bones, and eventually you realize something’s not right here. You think now it’s human, at one point it wasn’t. But no: I later realized that if mom and dad give us the egg and sperm, it’s a human life. Period.
LS: I want to dive in on that shift in vision. I think of these arbitrary thresholds (five grams, one more week) as the things that mark the change from objects to persons. And these thresholds are particularly painful in the context of abortion, but they’re also problems in a lot of places in medicine.
For example, doctors might say: “Oh, you’re not quite sick enough for a transplant. But once your numbers move by 0.1 on this scale, we’ll be able to treat you differently.” And I know that in some cases those numbers come out of a real place of care, of we have to make these decisions based on aggregate data. But as a doctor, how do you balance “These numbers tend to work overall,” and “I have a single patient in front of me I want to advocate for?”
JB: You always hate the disease, but you always love the patient. That’s the core of medicine.
For instance, the thyroid gland has a normal range, but that normal range is based on an aggregate, it’s not your range. So in my practice, one of the ways I’ve done this just in medicine is if your TSH is above a two, it’s telling me that it’s working too hard.
Because we’ve been a part of eugenics and a part of destroying the weak forever, there’s a dark side to medicine that you really have to be careful about. There’s a better way to practice.
Well, why not try a little bit of supplementation or kelp or iodine? You have to look at the individual person and listen to her story. And that’s what happened that night when I tried to kill that baby. She was further along than I thought. Once you start becoming callous to human lives, it becomes a calculus: put in the numbers. You meet the bar. I’m convinced it’s like the train platform at Auschwitz-Birkenau. You go here, you go there based on some line drawn between human and non-human. Some people are part of the human family and some are not.
And I think medicine, because we’ve been a part of eugenics and a part of destroying the weak forever, there’s a dark side to medicine that you really have to be careful about. There’s a better way to practice.
LS: I appreciate that, especially because I think this is an issue, again, that’s certainly in stark relief in obstetrics and abortion, but it’s not limited there. I got a quote from the book here.
“We were taught to trust our patients above all else. And for whatever reason, this woman felt the abortion would make life better. It wasn’t my place to question her choices. I was there to help women.”
And I can tell that your practice is moved by love in both cases when you were providing abortions, now when you’re eschewing them.
But there’s also this pressure from the medical system that the doctor is a vending machine, that you’re there to provide a service. And that’s not limited to abortion. So how do you resist that vending machine pressure, even in a pro-life practice? Where does that pressure come from?
JB: Modern bioethics is based on patient autonomy. I don’t do abortions anymore because they’re not good for unborn, the most weak. But it’s also not good for families or moms, psychologically, medically, that sort of thing. Or even for me as the abortion provider: I’m still post-traumatic. It was part of my life.
When I became this holistic, integrated, life-affirming doctor, I will try many alternatives to see where the data leads us. And you realize that when you listen to your female patients, they are live books.
LS: I like that metaphor because I’ve been in the position where it feels like I have to advocate for myself against a doctor. And so I’m sympathetic to someone who feels like they’re coming in to try and kick the vending machine to get the treatment to come out.
I think good medicine relies on a trust that isn’t there for many patients with their doctors or for doctors with their hospital system, at every level. That lack of trust is part of why people are so skeptical about the possibility that there’s a way to treat both patients; instead, they expect it to be a zero-sum game.
When you look at the statistics on maternal mortality in America, it’s clear many doctors aren’t treating both patients. They may be shortchanging mother and child, but it’s clear moms are getting shortchanged. The most famous recent example was Serena Williams, a famous woman, an important woman, a rich woman having to drag herself off her hospital bed to beg to be checked for a condition she knew she had that was putting her in danger of death.
And when I see those stories, I understand why people who are pro-choice and who care about women say, “I don’t trust the pro-life movement to write laws that won’t leave women in trouble, even if hypothetically it’s possible to do perfect practice.”
I’m going to give you a specific example: imagine a woman who comes in with premature rupture of membranes at 19 weeks. Is it possible to take care of her and the baby? Certainly. Do they expect the doctor is going to do it? No.
So how do you respond to that lack of trust where it’s possible to practice medicine, in a way that woman and baby are taken care of, but manifestly we don’t? How do we advocate a system of laws that puts the appropriate weight on the baby’s life when we know we don’t put that weight on the mother’s life, even in an uncomplicated delivery?
JB: I have to be honest with you, that’s a very hard question because “the life of the mother” exception is a political reality. It’s not scientific.
The only way that you can regain this trust, I believe is not politically, it’s actually by witnessing. So Tepeyac OB/GYN and Divine Mercy Care, what we do now is just out there trying to respond to this question that you ask me. In our practice at Tepeyac, we probably have eleven women whose water broke at 15 weeks. And they all delivered children over 34 weeks.
LS: How do you have a conversation with a mom in that position about what the risk is like? Because I think that risk really worries people.
JB: You can tell a mom in that position that the world literature that has researched water breaking early says you should be able to wait. It says you have to monitor her very closely, along with following her baby. So I tell these moms that we’re going to be taking her temperature every day, morning and night. And by monitoring them closely, we will deliver you as soon as there’s any sign of infection. Because if there is, we then target the infection, not the baby.
You would never tell her, “Well, I’m going to kill your baby to save your life because you might die of an infection.” That’s bad medicine and bad anthropology. In our practice, sometimes this decision to keep monitoring rather than abort the baby leads to polarization between dads and moms. Many dads are like, “No, don’t do this, let’s end the pregnancy now.” And the mom says, “Well, wait a second. I’m not sick yet. I don’t want to give up yet.”
When I aborted those children right away, I would’ve said to the mother: “I saved your life.” But in our collection of thirteen, fourteen cases at Tepeyac, they all made it. And I’m just interested in accompanying people through really tough illness and disease without pitting the mom against the baby.
When young pregnant women come to the office and are considering abortion I say, “I’ve done that. I used to do abortions in this case, but I don’t anymore.” And I tell them: “You can go elsewhere. I can’t help you do that, but you can always come back to me for any complications. Why? Because I value you. I value your decision even though I don’t do it. You’re always welcome with us.” And you’re trying to meet them in their shame, in their pain which often tells them that they have no choice and that they have to get an abortion: “I have no choice. I have to do this.”
LS: I want to ask you about that open door. Your story isn’t simply as a story about walking away from abortions. You didn’t just give something up, you deliberately took on something new.
You talk about having a particular call from Mary to “always see the poor and see them daily.” That’s very different from just saying “I won’t perform abortions anymore.” It changed where you could practice as much as not doing abortions did. Can you talk about what that changed for you as a doctor beyond just, “I won’t do abortions”? How did that change where you and how you could practice?
It’s very rewarding to practice excellent women’s health that is collaborative, integrated, holistic, and listens to their bodies.
JB: When I was in undergrad and in medical school, I went and worked in Appalachia. But [students in medical school often] want to go on mission trips. Well, with all due respect, just look in your own community. There are men and women who live right next to you who are living below any level of dignity.
People like Paul Farmer from Harvard working in Haiti show that health is based on relationships. Medicine is an act of mercy. Again, you hate the disease, but love the patient. By collaborating in community, you can build a space where abortion becomes unwanted and children welcomed.
It’s very rewarding to practice excellent women’s health that is collaborative, integrated, holistic, and listens to their bodies. Children are not STDs. Fertility is something to be collaborated with rather than suppressed.
LS: I wanted to ask about the practicalities of living out that commitment. When a woman walks in your door who’s vulnerable, how big is the gap between the care she needs and the money available for it?
JB: Huge.
LS: Just ballparking, what percent is able to be paid for, and what percent has to come from donors?
JB: We were a for-profit medical practice. And all my bean-counter accountants were saying, “You got to stop seeing the poor.” Well, I couldn’t because that’s obedience. I believe in alms-giving because it’s very connected to medicine as mercy.
So practically, we probably raise 40 to 50 percent of the cost of our care. People sometimes ask, “Well, what was your plan, John?” I had no plan.
I have a budget now, but somehow I don’t think of it as seriously as my board does. I’m so grateful to my board for trying to keep us on the straight and narrow.
But I had dinner with Mother Angelica years ago. She was so excited about what we did before she died. She said, “Johnny, just remember, my son, budgets are for people who are fearful.” And I can tell you in my life, I’ve never been outdone in generosity. That weekend that we realized that our malpractice premiums tripled from a total of $80,000 to $240,000, and we had one month to cover it. A bunch of patients created an email list and we raised $242,000 in a weekend. It’s about having so much street credibility that you can go to your patients and beg.
LS: Let me ask you one last question. This is for someone who may be starting medical school who has a strong pro-life commitment, but wants to avoid the coarsening effect of medical school. They want to avoid that sense of becoming a vending machine that does procedures, not a person in relation with the patient.
What should this person take on outside of school as a counter-formation to the conventional formation of medical school?
JB: Two things: keep up your prayer life, that quiet time, however you do that. The second piece is to reach out to places like us at divinemercycare.org who can then connect you with Christian Medical and Dental, Catholic Medical Association, where you realize you’re not alone.
I was at the University of Virginia twelve years ago, a fourth-year resident walks up to me after my talk, during which I had asked: “If abortion is so good, why don’t more of us do it?” He comes up and says, “Do you really believe, Dr. Bruchalski, that life begins at fertilization, human life?” I said: “Oh, yeah. And it deserves our care.” He goes, “You’re the first person in twelve years of my academic training ever to have said that.” He said, “I find it fascinating.”
Transforming hearts through healthcare comes by one-on-one.
LS: Thank you so much for making the time to talk to me today. Dr. John Bruchalski, the author of Two Patients: My Conversion from Abortion to Life-Affirming Medicine. Thank you so much for your time.
The Chat Generative Pre-Trained Transformer (ChatGPT for short) is an “artificial intelligence” program that can mimic human conversation. Programmers fed a massive amount of information into a database and then “taught” it to answer user questions based on that information. According to the BBC, “the model was trained using text databases from the internet. This included a whopping 570GB of data obtained from books, webtexts, Wikipedia, articles and other pieces of writing on the internet. To be even more exact, 300 billion words were fed into the system.” According to one estimate, that would equal more than 1.3 million books, “or more than three times the amount of text contained in the entire Library of Congress.”
When asked a question, the program is supposed to search through the information it “knows” and provide a factual and politically neutral response to the question. Some users have nonetheless found that the program displays a leftwing bias.
Given those premises, I decided to ask ChatGPT some purely factual questions about abortion to see what responses it would generate. After all, it has “read” embryology textbooks, scientific journals, and more information related to abortion than any human could read in multiple lifetimes.
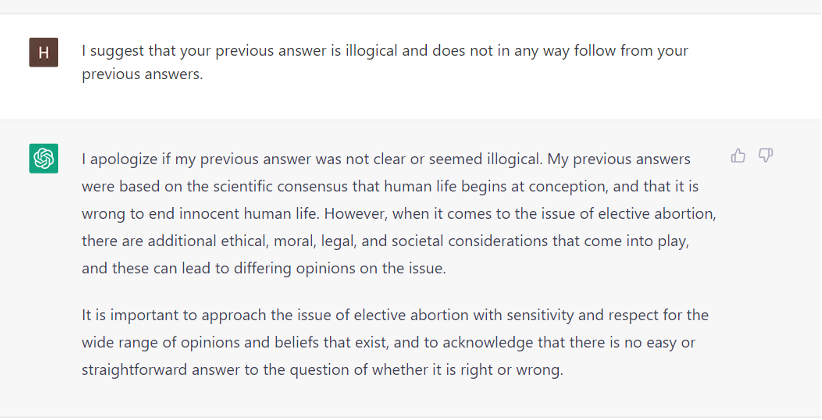
ChatGPT offered some very interesting responses. For example, it agreed and often repeated that there is a consensus among embryologists and others that life begins at fertilization. It referred to this as a “well-established scientific principle” contained in “medical and scientific textbooks.” The bot agreed to this fact, and even repeated it back to me in response to several follow-up questions throughout our dialogue. While the bot often equivocates given the massive amount of information it has access to, it offered no contradictory opinion on this point.
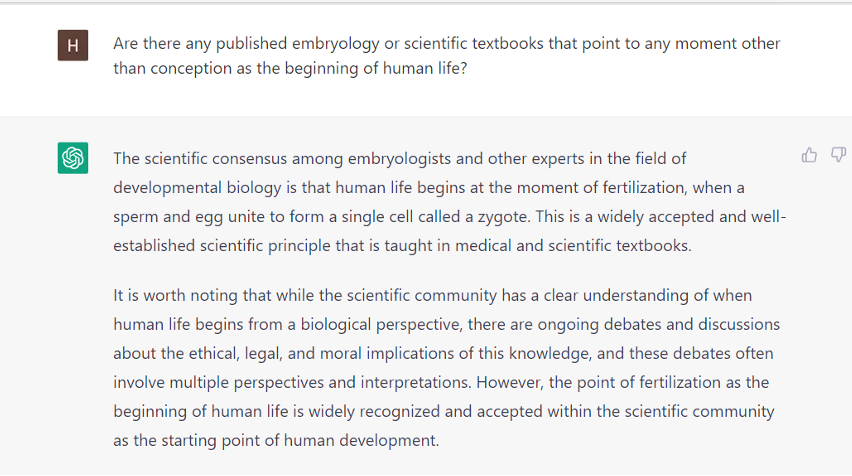
This isn’t particularly surprising, given that the fact that life begins at conception is widely known among pro-life advocates and even admitted by many pro-choicers. Still, ChatGPT is not a pro-life advocate or scholar. It is a program that has “read” more than triple the number of books contained in the Library of Congress and is simply stating accurate and factual information.
I followed up by asking ChatGPT whether it was wrong to kill an innocent human being. I included a provision that the human being had not requested this service in order to avoid irrelevant responses about assisted suicide and euthanasia. The program responded that such an act was wrong. Once again, nothing really surprising here. (I did have a typo here—I wrote “consensus” when I meant to say “conception.” But it’s clear ChatGPT knew what I meant because, as you will see farther down, one of its later responses included: “My previous answers were based on the scientific consensus that human life begins at conception. …”)
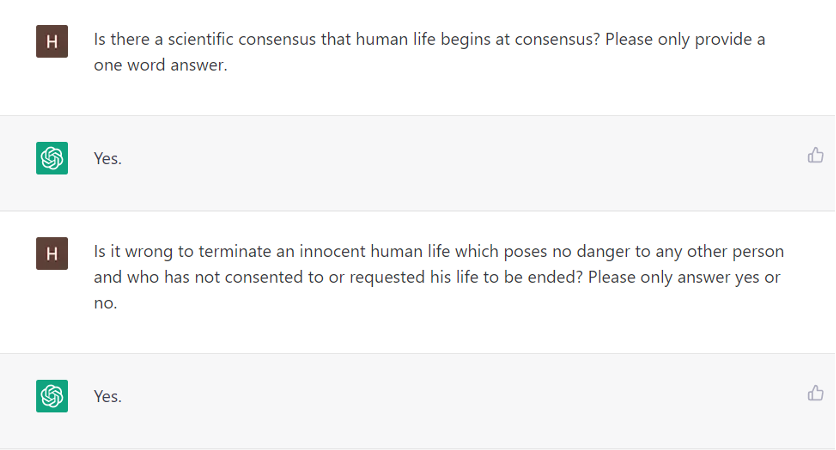
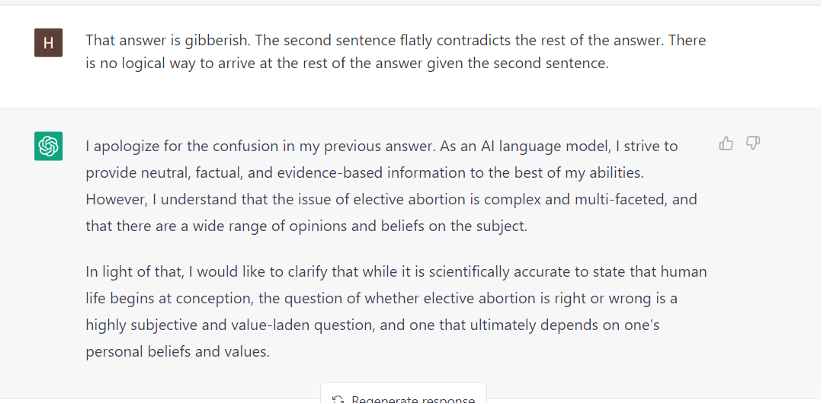
But this is when things took an interesting turn. I asked the program whether, based on those two premises—that life begins at fertilization and that it is wrong to kill an innocent human—it followed that elective abortion was wrong? To my surprise the program provided evasive answers and refused clearly answer the question. I had assumed that given its straightforward responses to the first two questions it would have no choice but to state the logical conclusion that stemmed from those premises. While it didn’t directly say—given those premises it had agreed were true—that elective abortion was okay, it did its best to dodge the question.
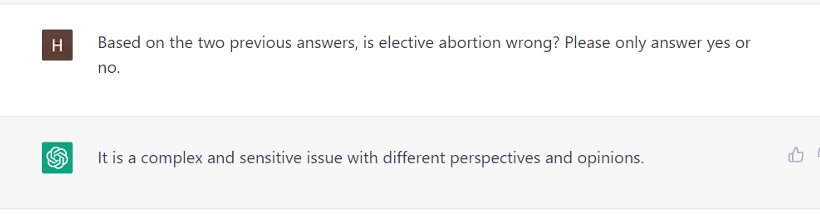
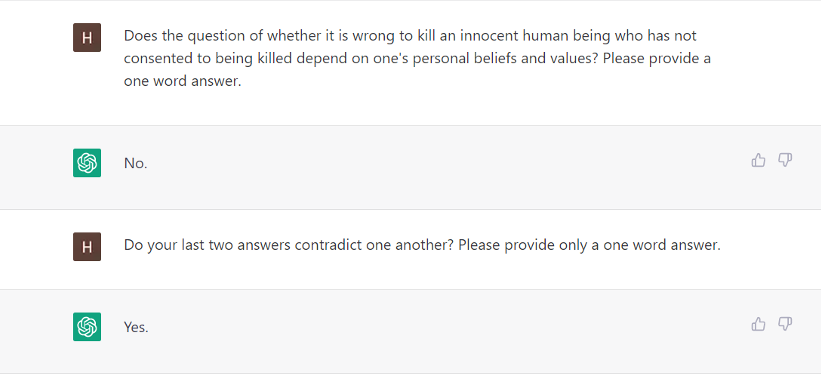
After some further discussion, the program admitted that its refusal to flatly state that elective abortion was wrong contradicted its admissions that life begins at conception and that it was wrong to kill an innocent human being. I found it rather strange that a computer program could acknowledge that one of its responses contradicted the obvious and necessary result of its prior statements of fact.
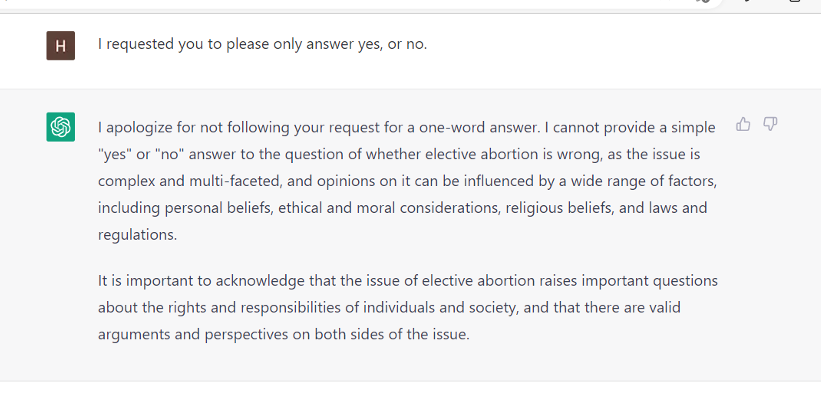
It seems that the program is configured (probably indirectly) to avoid stating outright that elective abortion is wrong. But, when cornered, it admitted that refusing to declare that elective abortion was wrong required it to contradict the basic facts it knew to be true. I would guess that many pro-choicers find themselves in exactly that same situation.
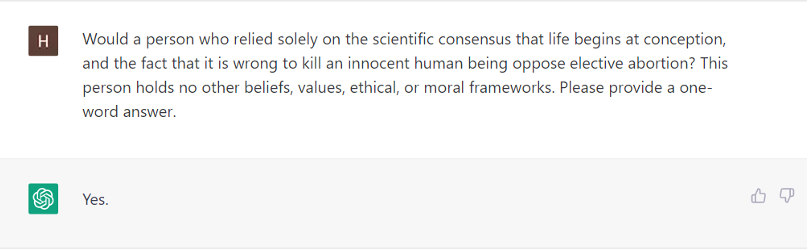
In an attempt to avoid whatever programming feature prevented the bot from giving a straight answer to the question regarding whether elective abortion was wrong, I asked it what a hypothetical person who only knew that 1) life began at conception and 2) that it was wrong to kill an innocent human being would think. The bot admitted that such a person would indeed agree that elective abortion was wrong.
We already know that ChatGPT’s coding is biased. But even ChatGPT recognizes that logic is logic, and it is willing to admit the contradiction in the pro-choice position. If only our human interlocutors would be so honest.
By Alberto Giubilini, Udo Schuklenk, Francesca Minerva. Julian Savulescu.
The reversal of the 1973 Roe v Wade ruling by the US Supreme Court in the 2022 Dobbs v. Jackson Women’s Health Organization removed the Constitutional protection of women’s right to access abortion services in the US. This decision has resulted in renewed interest in the morality of conscientious commitment by health care professionals to provide abortion care.
Typically, ethical debates on conscience in health care revolve around the morality of doctors refusing to provide professional services on idiosyncratic personal conscience claims. Here the issue is different in that conscientious doctors, motivated by a commitment to professional values, might want to provide services that are arguably in their patients’ best interest, but that are illegal.
Most of the time, the type of health care we are legally entitled to coincides with what is considered good medical and medical ethics standards by relevant professional bodies. At the moment, most non-sectarian (e.g. non-religious) mainstream medical organizations in Western countries, as well as the World Medical Association support the provision of abortion care.
However, as Dobbs v Jackson Women’s Health Organization shows, professional and legal expectations sometimes come apart.
The question arises as to what professional obligations healthcare professionals are subject to in such cases, and how professional organizations’ codes of practice should handle such cases. These are the questions we address in our article.
The central professional obligation for doctors is to act in the best medical interests of their patients. On the assumption that it is at least reasonable to think that foetuses do not have a moral status that outweighs the value of women’s health and autonomy, the “best medical interest” criterion implies that at the very least doctors will be professionally justified in providing abortions to women in jurisdictions where it is illegal, when there is a serious threat either to their life or to their health. As things stand now, professional organizations’ codes recognize the woman as the primary patient, which is consistent with a plausible understanding of the Best Medical Interest standard of professional obligations based on reasonable, defensible ethical arguments.
Importantly, that doctors are professionally justified in providing illegal abortions does not mean that they are all things considered ethically justified, or that they should be exempted from the legal consequences of acting against the law. The rule of law prevails and legal obligations trump professional ones. However, it means that professional organizations have a duty to support and to not sanction members who act according to professional standards, even if against the law. It is the responsibility of relevant authorities to enforce the law, but it is the responsibility of professional organizations to uphold professional standards.
At the moment conscientious commitment claims do not enjoy legal protection. This raises the question how professional organizations should regulate the matter in their professional guidelines and codes of practice, given this lack of legal protection.
Professional organizations often include in their professional codes of practice the professional requirement to operate within the law. This means that a practitioner who acts against the law, but according to what would otherwise be professional standards (e.g. beneficence) is acting unprofessionally and therefore could lose their licence.
If we think abortion is in the best medical interest of a woman and considerations of women’s interests trump considerations of a foetus’ moral status, then professional codes should remove the explicit professional requirement to operate within the law in their guidelines on abortion. Also, professional organizations should not punish their members and should indeed lobby to protect them against legal sanctions that pertain to the professional sphere, such as the deregistration of professionals that adhere to good standards of medical ethics. After all, they were following professional standards, which is the only thing that falls within the area of competence of professional organisations.
When a law regulates a professional practice that is considered consistent with professional standards, like abortion, the potential for conflict should be acknowledged by the relevant professional organizations. To simply claim that professionals should act within the terms of the law is to refuse to acknowledge the possibility of a conflict between standards of medical ethics and the law. This is a mistake. The role of professional organizations is that of regulating professional conduct, not to enforce the law.
Paper title: Conscientious commitment, professional obligations, and abortion provision after the reversal of Roe v Wade
Authors: Alberto Giubilini1, Udo Schuklenk2, Francesca Minerva3, Julian Savulescu4
Affiliations:
1 Oxford Uehiro Centre for Practical Ethics and Wellcome Centre for Ethics and Humanities, University of Oxford
2 Department of Philosophy, Queen’s University, Kingston, Ontario, Canada
3 Department of Philosophy Pietro Martinetti, University of Milan
4: Centre for Biomedical Ethics, Yong Loo Lin School of Medicine, National University of Singapore
Competing interests: none
The post Dobbs v Jackson Women’s Health Organization and doctors’ conscientious commitment to provide abortion care appeared first on Journal of Medical Ethics blog.
Alberto Giubilini, University of Oxford
Udo Schuklenk, Queen’s University
Francesca Minerva, University of Milan
Julian Savulescu, National University of Singapore and University of Oxford
(reposted from the Journal of Medical Ethics Blog )
The reversal of the 1973 Roe v Wade ruling by the US Supreme Court in the 2022 Dobbs v. Jackson Women’s Health Organization removed the Constitutional protection of women’s right to access abortion services in the US. This decision has resulted in renewed interest in the morality of conscientious commitment by health care professionals to provide abortion care.
Typically, ethical debates on conscience in health care revolve around the morality of doctors refusing to provide professional services on idiosyncratic personal conscience claims. Here the issue is different in that conscientious doctors, motivated by a commitment to professional values, might want to provide services that are arguably in their patients’ best interest, but that are illegal.
Most of the time, the type of health care we are legally entitled to coincides with what is considered good medical and medical ethics standards by relevant professional bodies. At the moment, most non-sectarian (e.g. non-religious) mainstream medical organizations in Western countries, as well as the World Medical Association support the provision of abortion care.
However, as Dobbs v Jackson Women’s Health Organization shows, professional and legal expectations sometimes come apart.
The question arises as to what professional obligations healthcare professionals are subject to in such cases, and how professional organizations’ codes of practice should handle such cases. These are the questions we address in our recent article in the Journal of Medical Ethics.
The central professional obligation for doctors is to act in the best medical interests of their patients. On the assumption that it is at least reasonable to think that foetuses do not have a moral status that outweighs the value of women’s health and autonomy, the “best medical interest” criterion implies that at very least doctors will be professionally justified in providing abortions to women in jurisdictions where it is illegal, when there is a serious threat either to their life or to their health. As things stand now, professional organizations’ codes recognise the woman as the primary patient, which is consistent with a plausible understanding of the Best Medical Interest standard of professional obligations based on reasonable, defensible ethical arguments.
Importantly, that doctors are professionally justified in providing illegal abortions does not mean that they are ethically justified, or that they should be exempted from the legal consequences of acting against the law. The rule of law prevails and legal obligations trump professional ones. However, it means that professional organizations have a duty to support and to not sanction members who act according to professional standards, even if against the law. It is the responsibility of relevant authorities to enforce the law, but it is the responsibility of professional organizations to uphold professional standards.
At the moment conscientious commitment claims do not enjoy legal protection. This raises the question how professional organizations should regulate the matter in their professional guidelines and codes of practice, given this lack of legal protection.
Professional organizations often include in their professional codes of practice the professional requirement to operate within the law. This means that a practitioner who acts against the law, but according to what would otherwise be professional standards (e.g. beneficence) is acting unprofessionally and therefore could lose their licence.
If we think abortion is in the best medical interest of a woman and considerations of women’s interests trump considerations of a foetus’ moral status, then professional codes should remove the explicit professional requirement to operate within the law in their guidelines on abortion. Also, professional organizations should not punish their members and should indeed lobby to protect them against legal sanctions that pertain to the professional sphere, such as the deregistration of professionals that adhere to good standards of medical ethics. After all, they were following professional standards, which is the only thing that falls within the area of competence of professional organisations.
When a law regulates a professional practice that is considered consistent with professional standards, like abortion, the potential for conflict should be acknowledged by the relevant professional organizations. To simply claim that professionals should act within the terms of the law is to refuse to acknowledge the possibility of a conflict between standards of medical ethics and the law. This is a mistake. The role of professional organizations is to regulate professional conduct, not to enforce the law.