Is a 15-week limit on abortion an acceptable compromise?
A recent opinion piece by George F. Will, “Ambivalent about abortion, the American middle begins to find its voice” in the Washington Post made the startling claim that the overturning of Roe v. Wade (Dobbs v. Jackson Women’s Health Organization, 2022) has resulted in “a partial healing of the nation’s civic culture.” One might think exactly the reverse. The Dobbs decision energized voters, especially women and young people, resulting in numerous Republican electoral defeats across the country. However, Will argues that the return of abortion policy to the states gives voters the opportunity of choosing moderate restrictions on abortion. Since most Americans support early abortion while opposing late-gestation abortion, Will thinks that a 15-week ban on abortion would be an acceptable compromise.
Why 15 weeks? Two reasons can be given. Almost all abortions in the US—93%—occur within the first 15 weeks of pregnancy. For this reason, making abortion illegal after 15 weeks would not, it would seem, impose serious burdens on most people seeking abortions.
Another reason is that several European countries limit abortion on request to the first trimester, leading some US lawmakers to suggest that a 15-week ban would bring our abortion law in line with theirs. This is disingenuous, to say the least. While elective abortion is limited in some European countries, it is not banned afterwards, but is allowed on other grounds, including economic or social reasons, or a threat to the woman’s physical or mental health. Moreover, in most European countries, patients do not have to pay for abortion; it is covered under universal health coverage. The fact is that the trend in Europe has not been to limit abortion, but to expand access to it. Countries in Europe “… have removed bans, increased abortion’s legality and taken steps to ensure laws and policies on abortion are guided by public health evidence and clinical best practices.”
Were states to guarantee access to abortion prior to 15 weeks, a 15-week ban might be acceptable. However, even before Dobbs, many women in the US lacked access to abortion, due to a dearth of providers, especially in rural areas. They often had to travel many miles to find an abortion clinic, which meant that they had to arrange childcare if they have other children or take time off work. Delay is also caused by the need to raise money for an abortion, which is not paid for by Medicaid in most states, except in cases of rape, incest, or a life-threatening condition. To be sure, even if there were none of these roadblocks, some women would still not be able to have early abortions because they do not know that they are pregnant, due to youth, being menopausal, chronic obesity, or a lack of pregnancy symptoms. Any time limits will pose hardships for some people. But if access to early abortions were guaranteed, a compromise on a 15-week limit might be worth it.
I suspect that time-limit advocates are not particularly interested in making sure that women who have abortions get them early in pregnancy. They want to place roadblocks in the way of getting abortions, full stop. That these roadblocks increase the numbers of late abortions is of little concern to them, however much they wring their hands over late abortions. Abortion can be reduced by reducing the number of unwanted pregnancies, something that has been shown to be achieved by access to contraceptives and science-based sex education in the schools. Remember when pro-lifers emphasized those methods? Me neither.
“Some US lawmakers suggest that a 15-week ban would bring our abortion law in line with European countries. This is disingenuous, to say the least.”
My second concern is with abortions sought after 15 weeks. The reason for a late abortion may be that the woman has a medical condition that has not developed, or has not been detected, until later in pregnancy. In such cases, the pregnancy is almost always a wanted pregnancy, and the decision to terminate imposes a tragic choice.
It may be responded that all states allow abortions to be performed when this is necessary to save the pregnant woman’s life, and many allow for abortions to protect her from a serious health risk. The problem is that these exceptions conflict with standard medical care, especially in the case of miscarriage. Once the woman has begun to miscarry, the failure to remove the fetus is likely to cause her sepsis, which can be life-threatening. However, in states with restrictive abortion laws, doctors cannot perform an immediate abortion, which is the standard of care in such situations. They have to wait until her death is imminent and, in some states, they cannot remove the fetus until its heart stops.
Ireland’s restrictive abortion law was repealed after a woman who was denied an abortion during a miscarriage died from septicemia. To the best of my knowledge, no woman in the US has died as a result of restrictive abortion laws, but some have come close. An OB-GYN in San Antonio had to wait until the fetal heartbeat stopped to treat a miscarrying patient who developed a dangerous womb infection. The delay caused complications which required her to have surgery, lose multiple liters of blood, and be put on a breathing machine. Texas law essentially requires doctors to commit malpractice.
Conservatives often portray those in the pro-choice camp as advocating abortion until the day of delivery, for trivial reasons. This is deeply unfair. If they want us to compromise on time limits, they should be willing to guarantee access to abortion before 15 weeks. They should be willing to compromise on pregnancy prevention through contraception and sex education. And they should agree to drop all restrictions on late-term abortions that make legislators, rather than doctors, in charge of deciding what is appropriate medical care for their patients.
Featured image: Gayatri Malhotra via Unsplash (public domain)
The new documentary “No Way Back: The Reality of Gender-Affirming Care” criticizes transgender ideology from a self-described “liberal, west coast Democrat” perspective. Despite facing significant resistance from trans activists, it has been making an impact.
The film will be showing in select theaters across the country during a one-day AMC Theatres Special Event on Wednesday, June 21st at 4:30 and 7:30 pm. It will be available online and on DVD starting July 2nd.
Below, Joshua Pauling interviews producer Vera Lindner.
Joshua Pauling (JP): Thanks for taking the time to discuss your new documentary. It really is a powerful depiction of what is happening to people when transgender ideology takes over. I especially found the detransitioners’ stories compelling. The story you tell throughout is decidedly reasonable and anchored to reality. Kudos to you all for producing such a thorough and moving documentary on such an important and controversial topic. And much respect for being willing to say hard but true things in the documentary.
How has the response been to the film thus far?
Vera Lindner (VL): We’ve received tons of gratitude, tears, and donations. The most humbling has been the resonance the film created in suffering parents. I wept many times reading grateful, heartbreaking messages from parents. People are hungry, culturally speaking, and are embracing our film as truth and facts, and a “nuanced, compassionate, deeply researched” project.
JP: That is great to hear, and interesting that there has been an overwhelming response from parents. Parents are frequently the forgotten victims of this ideology.
How has the film been doing when it comes to numbers of views and reach?
VL: Since February 18th, the film has been viewed 40,000 times on Vimeo, after it was shut down in its first week and then reinstated due to publicity and pressure from concerned citizens. Many bootlegged copies have proliferated on Odysee, Rumble, and such, so probably 30,000 more views there as well. After we put it on Vimeo on Demand in mid-April, it’s getting purchased about 50 times a day. Our objective is the widest possible reach.
Since February 18th, the film has been viewed 40,000 times on Vimeo, after it was shut down in its first week and then reinstated due to publicity and pressure from concerned citizens.
JP: Sad to say, I’m not surprised that it was shut down within a few days. Can you explain more about how such a thing happens? In what ways has it been blocked or throttled?
VL: Vimeo blocked it on the third day due to activists’ doing a “blitz” pressure campaign on Vimeo. Then they reinstated it, after news articles and public pressure. Our private screening event in Austin was canceled due to “blitz” pressure on the venue (300 phone calls by activists in two days). These experiences help us refine our marketing strategy.
JP: I guess that shows the power of public pressure, from either side. You know you’ve touched a nerve when the response has been both so positive as to receive countless heartfelt letters from people, and so harsh that activists want it canceled.
What do you see as next steps in turning the tide on this topic as a society? What comes after raising awareness through a documentary like this?
VL: Our objective was to focus on the medical harm and regret of experimental treatments. All studies point to the fact that regret peaks around eight to eleven years later. Yet the message of the activists toward the detransitioners is, “It didn’t work for you, you freak, but other people are happy with their medicalization.”
Our expectation is that conversations about the long-term ramifications of this medical protocol will start. We need to talk not only about how individuals are affected, but the society as a whole. Wrong-sex hormone treatment and puberty blockers lead to serious health complications that could lead to lifelong disability, chronic pain, osteoporosis, cardiac events, worsening mental health. SRSs (sex-reassignment surgeries) cost hundreds of thousands of dollars. These are not just one individual’s personal issues.
The economics of our health insurance will be impacted. The ability of these people to be contributing members of society will be impacted profoundly. The Reuters investigation from November 2022 stated that there are 18,000 U.S. children currently on puberty blockers and 122,000 kids diagnosed with gender dysphoria (and this is only via public insurance data, so likely an undercount). These all are future patients with musculoskeletal, cardiovascular, and mental illnesses for a lifetime. A hysterectomy at twenty-one can lead to early dementia, early menopause, and collapse of the pelvic floor organs.
The economics of our health insurance will be impacted. The ability of these people to be contributing members of society will be impacted profoundly.
I don’t yet see conversations about the long-term health implications of “gender-affirming care,” particularly in relation to how insurance, the labor force, interpersonal relationships, and future offspring will be affected. Everyone wants to be affirmed now and medicalized now. But there are lifelong implications to experimental medicine: autoimmune illnesses, cancers, etc. Sexual dysfunction and anorgasmia have real implications on dating, romantic life, and partnering up. A few people are talking about this on NSFW posts on Reddit.
JP: It’s interesting how speaking out against trans ideology and gender-affirming care creates some unlikely alliances across the political and religious spectrum. What do you see as the potentials and pitfalls of such alliances?
VL: We align with people who are pro-reality, who respect core community values such as truth and honesty, and who see the human being as a whole: body and soul. There is no metaphysical “gendered soul” separate from the body. Teaching body dissociation to kids (“born in the wrong body”) has led to a tidal wave of self-hatred, body dysmorphia, depression, anxiety, and self-harm. We are our bodies, and we are part of the biosphere. We respect nature and the body’s own intricate biochemical mechanism for self-regulation, the endocrine system. We believe that humans cannot and should not try to “play God.” We are students of history and know that radical attempts to re-engineer human society according to someone’s outrageous vision (read Martine Rothblatt’s The Apartheid of Sex) have led to enormous human cataclysms (communism, Chinese cultural revolution).
We are our bodies, and we are part of the biosphere. We respect nature and the body’s own intricate biochemical mechanism for self-regulation, the endocrine system.
JP: Well, then count me a realist, too! Funny you use the term pro-reality. I’ve written similarly about the possibility of realist alliances. While this makes for some improbable pairings, there can be agreement on the importance of fact-based objective reality and the givenness of the human body.
Realists can agree that the world is an objective reality with inherent meaning, in which humans are situated as embodied, contingent beings. Such realists, whether conservative, moderate, or progressive, might have more in common with each other on understanding reality and humanity than some on their “own side” whom I call constructivists: those who see the world as a conglomeration of relative meanings, subjectively experienced by autonomous, self-determining beings, who construct their own truth and identity based on internal feelings.
But I do have a related question on this point—a bit of respectful pushback, if I may.
Your pro-reality position seems to have implications beyond just the transgender question. Can one consistently oppose the extremes of gender-affirming care while upholding the rest of the LGB revolution? If our male and female bodies matter, and their inherent design and ordering toward each other mean something, then doesn’t that raise some questions about the sexual revolution more broadly?
As we see the continued deleterious effects on human flourishing unfold as thousands of years of wisdom and common sense regarding sex and sexuality are jettisoned, there are both religious and non-religious thinkers raising this question, though some go farther than others. I think, for example, of Louise Perry’s The Case Against the Sexual Revolution, Christine Emba’s Rethinking Sex, Mary Harrington’s Feminism Against Progress, and Erika Bachiochi’s “Sex-Realist Feminism.” An enlightening panel discussion with many of these thinkers was co-hosted by Public Discourse earlier this year. When the real human body is considered, its holistic structure as male or female is clearly ordered and designed to unite with its complement.
If our male and female bodies matter, and their inherent design and ordering towards each other mean something, then doesn’t that raise some questions about the sexual revolution more broadly?
How does this reality relate to the rest of the sexual revolution? If one argues that individuals should be able to express themselves sexually and fulfill their desires with no external limits beyond human desire or will, how does one justify saying that transgenderism is off-limits?
VL: I will answer the question, but I need to say that this is my personal opinion. I’m fifty-five and have worked in entertainment for more than thirty years, and in Hollywood for twenty-five years. The entertainment industry attracts LGBT people, so I’ve hired, mentored, befriended, and promoted LGBT and gender-non-conforming people every day of my career. I believe that being gay or lesbian is how these people were born. Some were affected by their circumstances, as well, but in general I believe that homosexuality is innate, inborn, and has existed for millennia. There were a handful of “classic” transsexual women as well. I have three close friends who transitioned in their late forties.
But the explosion we are seeing now is different. A 4,000-percent increase of teenage girls identifying as trans? This is unprecedented. Mostly these are autistic, traumatized, mentally ill teens who seek to belong, who wish to escape their traumatized brains and bodies, who have been bullied relentlessly (“dyke,” “fag,” “freak”) and now seek a “mark of distinction” that will elevate their social status. Instead of being offered therapy, deep understanding, and compassion for their actual traumas, they are being ushered toward testosterone, mastectomies, and hysterectomies. This is not health care. The tidal wave of regret is coming, because these adolescents were never transsexual to begin with. Many of them are lesbians or gay boys who have internalized so much homophobia and bullying that they would rather escape all of it and become someone different than deal with it.
This is what we want to address. Kids explore identities. This is a natural process of discovering who they are. Medicalizing this exploration cements this exploration they were doing when they were teens. Life is long, and one goes through many phases and many “identities.” To be “cemented” for a lifetime in the decision you made as a distressed sixteen-year-old to amputate healthy sex organs does not make sense.
JP: The rise in the rate of transgender identification is indeed stunning, as is the stark increase in the percentage of Gen-Zers who identify as LGBT. What those trends portend is a live question, as are the varied possible causes. And as you say, there is a tidal wave of regret building, from those who have been pushed toward gender transition. We will all need to make special effort to love and care for them.
You’ve been so gracious with your time. As we conclude, are there any other comments you’d like to share with our readers?
VL: Find a theater near you to attend the theatrical one-day premier on June 21st. Then the movie will become available online and via DVD on July 2nd. Watch the documentary and pass it on to all in your circles!
And ask commonsense humanistic questions:
– Can adults make decisions on behalf of kids that will forever change the path of the kids’ lives?
– Is it worth it to ruin one’s health in the name of a belief system?
– Is what you are reading in academic medical research based on evidence, or pseudo-science?
– If humans have been going through puberty for millennia, who are we to mess with that now?
– Is puberty a disease?
JP: Thank you for your work on this vital issue. I hope this documentary continues to make an impact. And realists unite!
By Rebecca Farrington, Louise Tomkow, Gabrielle Prager, and Kitty Worthing.
Healthcare professionals are increasingly expected to be hardy and ‘suck it up’ to survive in complex and demoralising workplaces. As NHS clinicians, we saw staffing shortages and limited resources firsthand during the COVID-19 pandemic. These experiences magnified our scepticism about the onus on us, as individuals, to be ‘resilient’ as a solution to both the workforce crisis and wider societal problems.
Our paper ‘In critique of moral resilience’ describes the responses of NHS staff faced with navigating COVID-19 and caring for one of the most disadvantaged groups in our society – people seeking asylum housed in contingency accommodation. The staff we interviewed provided a social commentary on the state-sponsored neglect of vulnerable migrants in the UK. We don’t overlook this, but we focus on healthcare professionals’ understanding, responses and negotiation of their roles in this ‘Hostile Environment’.
Resilience was clearly important to staff for self-preservation, but so was an ability to see the limits of a biomedical approach to social suffering. The concept of moral resilience helped to unpick this but was not enough to describe the ideological changes and challenges to systems made by staff using their new insights. They did put up with the difficult bits of their work, and we describe how they survived. However, these coping actions alone did nothing to change the status quo in the political and social systems causing the underlying health problems. Some staff we interviewed made positive changes in the lives of the people seeking asylum through activism to improve their health and wellbeing. We found that the concept of resilience failed to capture these important moral actions: advocating beyond the clinic, beyond just doing their best on the job.
The popular focus on resilience is here to stay in much of our work and home lives, but we encourage caution in using it as a broad-brush solution to complex problems. Healthcare providers who see and yet continue morally problematic care in the name of resilience might be thought of as complicit in social suffering. Does moral resilience just promote acceptance of the status quo, even when it feels unbearable? What cost does this fixation on resilience bring to both care providers and patients?
Reflecting on our work in clinical medicine, research, and medical advocacy, we recognise that some of our most effective improvements to social conditions have been through collective action and joint resistance. In times of increasing moral outrage, such as against the UK government’s illegal migration bill, this feels a more appropriate response than just sucking it up in the name of resilience in the hope that we will survive.
Authors: Louise Tomkow1, Gabrielle Prager1, Kitty Worthing2, Rebecca Farrington1
Affiliations:
The post Does our preoccupation with resilience mean we must tolerate the morally intolerable? appeared first on Journal of Medical Ethics blog.
![]()
In a piece that stares down tragedy and refuses to give up, Jen Agg recounts the agonizing weeks following her husband’s stroke, which took place at the onset of the pandemic. This is a gripping essay about being strong for someone else, but it’s also a piece about the devils and angels in the medical system: those who think dashing your optimism is some sort of sadistic duty vs. those who understand their role is to offer not only medical help, but most importantly, kindness and hope.
I started describing a stroke as a twenty-car pile-up on the highway of your brain’s quickest route. Recovery is the next car getting off the highway just before the devastation and twisted-up metal of cars blocking the road, except it’s night time, and the power is out, and it’s a thunderstorm and actually, turns out there is no road. So one car slowly and timidly draws a new path where there never was one. Your brain is resourceful this way, but it’s slow going. After a while, all the cars start taking this newly formed exit and your brain learns a whole new way of communicating with your body.
At first it was the destabilizing uncertainty: would it be a bad day, or a rare good day? How could I keep both our moods afloat when I was working really hard on the basics of our survival while maintaining an unbreakable facade of hopefulness? Was there effort in that? I don’t remember. Roland was sad a lot at the beginning and I knew I couldn’t let that sadness drown us both. Many of life’s challenges force reaction and demand a change of perspective, but particularly with health issues, you have to really be committed or the ugliness of it can win. I absolutely refused to let it. This was not going to be the thing that unwound our love—a love born in a fireball of attraction, bonded over a shared enemy and nurtured over decades of simply never being bored of each other or running out of fascinating things to talk about while remaining enthralled with each others’ faces.
By Abeezar I. Sarela.
In its recent guidance on consent, the General Medical Council (GMC) advises doctors to not provide treatment that ‘you (the doctor) don’t think would be in their (the patient’s) clinical interests’. It follows that doctors should only provide treatments that are in the patient’s clinical interests. But, what exactly is meant by ‘clinical interests’?
The GMC does not explain the term. In practice, it is sometimes confused with ‘best interests’. However, best interests is a legal term that applies specifically to making decisions for people who lack the capacity to do so for themselves. For example, oncologists might consider that either chemotherapy A or chemotherapy B could be in the clinical interests of a patient without capacity. Best interest decision-making would then involve choosing between A and B, or avoiding any chemotherapy and giving supportive care only. Whereas, patients with capacity would make these choices for themselves and do not need others to decide their best interests.
The difference between clinical interests and best interests is similar to that between setting a menu and then choosing from that menu. Clinical interests set the menu of treatment options that is available to a patient. Patients can then choose any option from this menu or decline all options, regardless of the consequences, because we all have a right of self-determination. But, do patients have a right to participate in setting the menu, too? Some might say yes. They would argue that treatment availability comes down to a matter of informed consent, through a process of shared decision-making (SDM) between the doctor and the patient.
However, senior judges have been clear that consent is valid only if the proposed treatment is, in the first place, ‘proper’. If the treatment is not proper, then the patient’s consent is meaningless, regardless of the sharing of information. In other words, setting the menu is not a matter for SDM. Rather, informed consent has two distinct stages. In the first stage, the doctor has to identify treatments that are proper (reasonable or available) for that patient. Then, the doctor has to involve the patient in the choosing between available treatments (or not having any treatment). It is this second stage that requires SDM: a dialogue about the menu of available treatments from the first stage.
What is it that makes a treatment available in the first place? Judges have explained that for a treatment to be available it has to be in the ‘public interest’. This turn to public interest can be justified in various ways. In a civilised society, we all (the ‘public’) have an interest in each other’s welfare. And, in some cases, the public interest can override an individual’s own wishes. Furthermore, in a publicly-funded health service it is inescapable that making treatment available to one person reduces resources for others. Consequently, it is in the public interest to set limits on availability of treatment.
The GMC would seem to have re-phrased ‘public interest’ as ‘clinical interests’. The endpoint of both is the same: the identification of available treatments. Thus, in advising doctors to think about a patient’s clinical interests, the GMC is actually asking doctors to consider the public interest. The GMC leaves this task to the professional judgment of doctors; and judges have done similarly. This approach is consistent with a well-established sociological argument that the public grants the medical profession with the authority to make certain decisions on its behalf. As doctors, let’s celebrate this sociological mandate and strive to serve the public. Or let’s challenge it, and find an alternative way. But, in the meanwhile, let’s not hide behind smokescreens of SDM and consent to decide about the availability of treatment.
Author: Abeezar I. Sarela
Affiliation: Department of Surgery, The Leeds Teaching Hospitals NHS Trust.
Competing interests: None declared
The post Re-thinking consent for treatment: clinical interests and the public interest appeared first on Journal of Medical Ethics blog.
The battle against transgender ideology will be won by the wounded.
Chloe Cole’s recent discussion at the Heritage Foundation shows that the victims of the transgender movement are the ones who will defeat it. The eighteen-year-old is a flesh-and-blood refutation of the supposed medical authority and scientific expertise of the trans movement. The wounded bodies and psyches of detransitioners rebut the trans movement’s claims to compassion and expertise. Their scars are marks of its fallibility, and their existence shows that the science is not settled. They are living proof that the affirmation-only approach is hurting people.
But sending them to the frontlines of the fight against transgender ideology—and against the medical-pharmaceutical complex that profits from it—is asking a lot from those who are already hurt. The courage of Chloe’s testimony is evident in the vulnerability it requires to share intimate details about her body, her mental health, and her social and family life. The cost of telling the truth about transition is surrendering a lot of privacy. For example, Chloe related that “after about a year or so being on testosterone I started experiencing some urinary tract side effects. I was more prone to getting UTIs [urinary tract infections] and sometimes I would even get blood clots in my urine.” Few adults would want talk about this on a national stage, especially as part of a heated culture-war debate. Yet she is doing this while still a teenage girl.
This youthful courage in turn highlights how very young she was when the medical profession endorsed her internet-induced trans identity and began altering her body through puberty blockers, testosterone, and surgery.
She was only fifteen when they amputated her breasts. This surgery was done on the theory that children can know themselves to be born in the wrong body, and that in such cases total affirmation, including medical transition, is the best treatment. Indeed, activists, including doctors and therapists, often present transition as necessary to prevent suicide—transition the kids before they kill themselves. This was the line given to Chloe’s parents, who were reluctant about her transition. But as Chloe said, “they were told that if I wasn’t allowed to transition as I pleased I would have been at risk of suicide.”
Her worried parents were right to be reluctant, and the supposed experts were wrong. Chloe’s transgender identity was not the product of an innate, immutable gender identity, but the result of being an awkward young girl under the influence of the internet. As she explained,
I didn’t really get along with the other girls and I started to wonder what exactly was setting me apart from them. I started to become a little bit insecure about this and I also started developing some body issues. . . . I started using social media after I got my first phone at eleven; the first platforms I used were primarily Instagram and Snapchat. Both of those are very image-oriented, and I would see a lot of very, you could say, idealized or sexualized images of adult women and young women on there . . . that I didn’t really match up to. . . . [C]ompared to other girls I felt like I looked like a boy and it just felt like I couldn’t really match up to other women.
But there is a way out of the unrealistic expectations that our toxic culture pushes on girls: stop being one. The social media algorithms helped send this message to Chloe, pushing a torrent of pro-trans content at her.
This dynamic, in which a poisonous environment for young women makes transition more appealing, was also present offline. Chloe related how, after she had begun transitioning, there was a bully who “one day towards the end of the school year, he actually sexually assaulted me; he groped my chest. . . . I never really thought that anybody would notice that part of me, but he did, and he took advantage of me and I wanted to hide that part of me for the rest of my life. I didn’t want anything to do with it, and I didn’t want the attention that I thought it would bring me.” She tried to ignore the assault, but the trauma of it pushed her further toward having her breasts amputated, which was done within two years of the incident.
Transgender activists and their allies have had it all their own way, and are now insisting that the science is settled.
Chloe’s experience illuminates why there has been an enormous increase in adolescent girls claiming to be transgender. This surge ought to raise red flags even among those who otherwise accept the claims of gender ideology, but it has been largely brushed off. Chloe’s story shows how gender ideology offers these girls an explanation for, and a way out of, the awkwardness and discomfort of female adolescence—difficult times that are being made much worse by the internet. Social media ensure constant comparison to, and judgment by, what seems like the entire rest of the world. And, as in Chloe’s case, there are the sexual abuses and assaults that many young women suffer. No wonder these girls don’t want to be themselves anymore.
Furthermore, there is very weak evidence to support the claim that the psychological distress of gender dysphoria should be treated with permanent chemical and surgical bodily modification. That this idea has organizational backing from medical associations just provides a perfect example of how professional groups can be captured by a determined band of activists whom no one wants to offend. Other than activists or the ambitious (or academics, who tend to be both), most doctors are too busy to bother much with the groups that represent and regulate their profession. And so transgender activists and their allies have had it all their own way, and are now insisting that the science is settled. They are even trying, with success in some states, to ban any alternative to the affirmation-only model of treating children who claim to be transgender.
But the science isn’t settled, as Chloe Cole and a multitude of other detransitioners prove. In her case, though she didn’t realize it at the time, “it was actually my transition that was worsening issues that were going unaddressed, or even creating new issues.” For instance, though she could now pass as male, she was still attracted to boys, which meant that “my dating pool was pretty restricted and this was a major point of distress for me over the years . . . I was really insecure about this since I had a lot of shame and I felt lonely.” Transitioning had not solved her social or emotional problems, and she began realizing that it had been a mistake. She began to privately experiment with living as a young woman again: “I didn’t live as a girl and I didn’t have breasts anymore but in the comfort of my room or whenever nobody was home I would—I bought some skirts and dresses and my old girl clothes in secret and my feelings about this just got worse over time and I never really talked to anybody about it.”
But she found her courage, first to tell her family, and then to tell the world. The stories of Chloe and other detransitioners are the ultimate rebuke to the arrogant claims of activists and the medical groups they have captured. It is, of course, also important to point out all the flaws in the studies trans activists cite, from poor design to small sample sizes to follow-up loss to short time frames. We should also note that many studies are inapplicable to our situation; studies of carefully screened European adults are unlikely to predict much about American adolescents who are getting cross-sex hormones after a single telehealth appointment. But no intellectual critique can match the condemnation of transgender ideology that is presented through the wounded bodies of patients who have been mutilated by their own doctors. Claims of compassionate expertise wither before their scars and stories.
It is not just that the transition regime of surgery and chemicals has left Chloe with “complications years after the fact, some of which have popped up just last year,” though the high rate of complications and side effects from medical transition is a scandal. Rather, it is also that transitioning took things from her that she, as a child, was utterly unable to give informed consent to. She related how painful it was to learn that “breastfeeding is a major part of building the bond between mother and child and that that bond will later affect a child’s social and emotional and cognitive development and I realized that when I got my breasts taken away there was so much more that was taken away. . . . I felt like a monster.”
But Chloe is not the monster. The monsters are those who are encouraging children to chemically sterilize themselves; the monsters are those who are profiting from amputating the healthy breasts of confused adolescent girls. And by showing everyone who the real monsters are, detransitioners provide support for the many additional victims of transgender ideology. The supposed urgency of affirmation been used to dismiss the claims of other victims, especially women and girls who have lost rights and opportunities as trans-identified men push into female spaces. Female athletes have had to compete against men; female prisoners have had to share cells with men—including violent rapists—and girls and women across America can no longer assume that their locker rooms, bathrooms, and changing rooms are for women only.
The monsters are those who are encouraging children to chemically sterilize themselves; the monsters are those who are profiting from amputating the healthy breasts of confused adolescent girls.
Additionally, there are the parents who have had their rights violated or lost their children to this ideology. There are the many people who have been punished or threatened for questioning gender ideology in their workplace. And there are many more, from the academy to Wall Street to the union hall who have been intimidated into silence as gender ideology has swept through American culture and institutions.
Transgenderism is culturally powerful and financially lucrative—every troubled teenage girl who identifies as trans is worth a fortune to the medical–pharmaceutical complex. Greed and ideology are a potent combination, so it is no wonder that almost all safeguards have been abandoned when it comes to transitioning children.
But this greed may be their undoing. Just as the stories of those who have detransitioned disrupt the transgender narrative, their lawsuits may bring down the medical and pharmaceutical cartels that profited from hurting them. The transgender monolith will fall as its victims stand up to it.
Horse paste has struck out again: even at high doses, ivermectin is "futile" as a treatment for Covid 19, according to a large double-blind trial published in JAMA.
— Read the restThe median time to sustained recovery was 11 days in both the ivermectin and placebo groups (hazard ratio [HR], 1.02).
![]()
By Karel-Bart Celie.
In a recent issue of JAMA, Ahmed et al. published data on healthcare unionization in the United States between 2009 and 2021. Despite the observed association between unionization and higher wages, better benefits, and more equitable compensation, unionization among healthcare workers has evidently remained low. Richman and Schulman (R&S) wrote a commentary focused specifically on unionization by physicians. They argued that physician unionization helps (1) restore some governance of healthcare systems and (2) provide a mechanism by which to deploy professional ethics in the service of patient welfare.
To the first point, more than half of all U.S. physicians are now employed by hospitals or other health systems. This shift in the landscape has resulted in a decrease in “professional sovereignty” threatening the loss of professional independence—something unionization might help prevent. Regarding the second point, leaders of large health systems have at best a divided loyalty; they are obligated to prioritize the fiscal concerns of their institutions. For example, one way to maximize profits is to minimize staffing despite a burned-out workforce and evidence that such practices can lead to worse outcomes. Physicians, on the other hand, have less of a commitment to the financial bottom line of the institution. And in any case, deeply-ingrained professional ethics serve as a corrective that “counters market incentives.” Unionization provides physicians with a “means to exert influence” on large health systems, in a manner that reflects the profession’s dedication to patient welfare.
I agree with these points and would like to submit two additional observations.
First, the age-old call to “at least do no harm” cited by R&S, which appears in Book I of the Epidemics, is often interpreted in relation to patient care. However, there is also a contextual argument for a similar duty to colleagues in the Hippocratic corpus. The Hippocratic Oath devotes a sizeable second paragraph to describing the respect and care with which one should treat one’s teachers and pupils. This paragraph accounts for nearly a third of the total text, and exhorts its reader to regard both teachers and pupils as family. It serves to remind us that our duties are not only to patients, but to each other as well. This is an aspect that is under-emphasized, to the detriment of a profession that is so inexorably collegial. How we consult with physicians from other specialties, with nurses and other allied staff, and with those who are learning from and teaching us, all have an impact on “the profession” and how its values are applied. The doctor-patient relationship—recipient of much attention—exists only in the context of physicians who constantly learn from, teach, and interact with each other.
The communal aspect of our professional ethics is obliquely understood, for example, when reporting unprofessional conduct. However, we do not have to stop at the negative. Physicians are accountable to each other in a positive sense also. Unionization is one way of giving this positive, intra-professional obligation a voice. It does so by promoting an environment of mutual support, collegiality, and legitimate concern for the wellbeing of members of the profession.
Second, housestaff unionization merits special attention at a time when burnout and depression remain prevalent among trainees in medicine. Unions help ensure fair wages and benefits; at my institution, wages for first-year doctors have risen by 15% since 2020. The accrediting body for graduate medical education (the ACGME) in the U.S. has increased initiatives to improve wellness in graduate medical education since 2017. However, it wields its punitive power over residency programs which are often themselves under pressure of the demands put upon it by institutions. Residents and their teaching faculty are often together in the proverbial “trenches.” Complaints to the ACGME are therefore challenging and often last-resort options for help, since everyone knows that doing so may simply shift the burden to another demographic (e.g., by removing trainees from a rotation, the same patient volume falls on the remaining faculty). Take for example the rule—a definite step in the right direction—that trainees are to work no more than 80 hours per week (caveat: averaged over 4 weeks!). Environments with low levels of staffing and high patient volumes virtually guarantee unacceptably high housestaff work hours. How could it not, especially where patient care is prioritized? Unions by contrast are more capable of addressing root causes, such as low levels of staffing, by directly confronting institutional stakeholders without necessarily compromising patient care. They also have the potential to spur legislation which holds institutions accountable for the treatment of their staff.
It is also important to note that housestaff unions can have a direct impact on improved patient care. The Patient Care Fund (PCF) was established by the Committee for Interns and Residents (CIR) in Los Angeles County in 1975 as a funding mechanism for trainee-driven improvements in patient care equipment. Since then, similar funds have been established by CIR across the country. In the last three years, housestaff from my own division have acquired a combined pulsed dye laser (PDL) and neodymium yttrium aluminum garnet (Nd:YAG) laser for burn reconstruction, as well as a new microscope for free flap reconstruction and digital replantation. All together this equipment represents nearly $300,000 invested in patient care at one of the busiest county hospitals in the country.
In summary, unionization by physicians in the U.S. provides a mechanism for us to apply our professional ethics, and thereby honor our (underemphasized) duties to each other. As a surgical trainee, I have also found that unions hold the potential to provide a more direct path to housestaff wellness than those currently afforded by educational organizations. For these reasons physician unionization merits continued support, despite the low rates reported by Ahmed et al.
Author: Karel-Bart Celie
Affiliations:
Competing Interests: None declared
Social media accounts of post author: Instagram @celie.md
The post Housestaff unionization in the United States and our duties to each other appeared first on Journal of Medical Ethics blog.
Canada has recently been in the news due to its imminent legal expansion of assisted suicide to include the mentally ill, beginning in March 2023. The Canadian government specifies that an “expert panel” will be used to evaluate the requests of the mentally ill “in a safe and compassionate way.” The virtue of compassion, which the Canadian government here invokes on its own behalf, is concerned with the best interests of the sufferer. So the question naturally arises: is it really “compassionate” for the state to offer death as an aid to the sufferer? Is it just?
To answer these questions, one must consider the state’s duty to its citizens. On this topic, there are few better guides than the Roman statesman and philosopher Cicero. Some things he gets right (the state’s duty to preserve justice and protect the well-being of its citizens) and others he gets wrong (the occasional permissibility of suicide). But if Cicero’s teachings are supplemented with Christianity’s teachings on suicide, we get a clear understanding of why assisted suicide cannot be counted among the state’s duties to its citizens.
If Cicero’s teachings are supplemented with Christianity’s teachings on suicide, we get a clear understanding of why assisted suicide cannot be counted among the state’s duties to its citizens.
In Book 1 of On Duties, a truly indispensable landmark in the history of political ethics—and Cicero’s last philosophical composition—Cicero says this (all translations in what follows are my own):
Absolutely all those who intend to preside over the commonwealth must observe Plato’s two precepts: first, that they guard what is useful for the citizens in such a way that they refer all of their actions to it, having forgotten about what is advantageous to themselves. Second, that they care for the entire body of the commonwealth, lest, while they guard some part of it, they abandon the rest. (On Duties 1.85)
Prima facie, this perhaps lends some support to the Canadian government. After all, those who are seeking death certainly believe that that is what is most useful to them; the government is merely assisting them in obtaining what they find useful. This would appear to fulfill Plato’s first precept as Cicero describes it.
And indeed, when it comes to suicide, Cicero allows that it is sometimes licit when done for the sake of honor. In On Duties 1.112, he points to Cato the Younger’s preference of death to subjection to Julius Caesar—“since nature had bestowed unbelievable seriousness on him”—as an example of honorable suicide. So if the magistrate is responsible for safeguarding what is advantageous for citizens, perhaps virtuous suicide should be legal. In other words, can suicide be both honorable and useful?
To answer this question, we must consider how honor relates to expediency.
Cicero devotes the third and final book of On Duties to showing that the useful and the honorable are never in conflict. If they were, injustice might sometimes be advantageous, as Thrasymachus argues in Book 1 of Plato’s Republic. But Plato has Socrates argue that any such advantage is merely apparent, for acting unjustly harms both the perpetrator and the victim. Cicero stands in this broad Socratic tradition: the one who commits an injustice for the sake of advantage is prevented from being a good man (On Duties 3.76); his victim suffers the consequences in his life, his property, or his reputation. Furthermore, unjust actions destroy fellowship among human beings, and thus contradict our very nature as social creatures. Therefore, they can never be useful.
Even if someone’s self-slaughter seems convenient and advantageous—perhaps because his suffering is great, or because his quality of life is low—it can never be so since it is unjust.
From the foregoing discussion, it becomes clear that the state cannot facilitate suicide without committing a grave injustice. Despite Cicero’s exemption for honorable suicide, even these are not just: all suicide is by definition the extrajudicial killing of a person who, in legal terms, is innocent. Cicero is right that the useful and just, ultimately, cannot conflict. Therefore, even if someone’s self-slaughter seems convenient and advantageous—perhaps because his suffering is great, or because his quality of life is low—it can never be so since it is unjust.
Here, Christianity’s tradition of political and moral reflection can provide further guidance. The late Roman church father Augustine takes up the question of suicide in the first book of his City of God in dealing with the question whether consecrated virgins who had been raped had justification for killing themselves. The question may strike modern ears as absurd, but it was not a crazy one at the time given that the Roman tradition answered questions like this in the affirmative, as the example of Lucretia shows.
But Augustine disagrees with his Roman forebears on the basis of the Ten Commandments of the Old Testament and the Two Great Commandments of the New Testament. He remarks,
For it is not for nothing that nowhere in the Holy Scriptures can we find God commanding or permitting us to inflict death upon ourselves either for the sake of gaining immortality or for the sake of keeping or freeing ourselves from any evil. For in fact it must be understood that we have been prohibited from doing this when the law says, “You shall not kill,” especially because it did not add, “your neighbor,” as it does when it forbids bearing false witness: “You shall not,” it says, “bear false witness against your neighbor.” Nevertheless, it does not provide grounds for someone to think himself innocent of this crime if he has borne false witness against himself, since he who loves has received the rule that guides the love of one’s neighbor from himself, since it has been written, “You shall love your neighbor as yourself.” (City of God 1.20)
In this passage, Augustine draws attention to two of the Ten Commandments: “You shall not kill” (or “murder”) and “You shall not bear false witness against your neighbor.” He notes that the latter includes a qualification that the former does not, and yet this does not mean that one can bear false witness against oneself; such dishonesty would obviously still be wrong.
Why? Because self-love—that is, the high regard in which we naturally hold ourselves—provides the standard for the love of one’s neighbor: “You shall love your neighbor as yourself.” If we are forbidden to tell lies about our neighbor, then we are by implication forbidden to tell lies about ourselves because of the necessary ethical link between treatment of self and treatment of neighbor.
If we were explicitly forbidden to kill our neighbor, we would by implication also be forbidden to kill ourselves, and the latter prohibition would be the ethical and logical foundation of the former.
In the same way, if we were explicitly forbidden to kill our neighbor, we would by implication also be forbidden to kill ourselves, and the latter prohibition would be the ethical and logical foundation of the former. But the commandment against killing does not even offer the kind of apparent grounds for casuistry that the commandment against bearing false witness does, because no qualification is made with respect to one’s neighbor. It simply states that all unjustified killing is wrong, with no exceptions—including killing oneself. Therefore, suicide violates the Ten Commandments. Not even Cato, says Augustine, is off the hook.
The Ten Commandments are especially helpful in this discussion because they are summaries of the moral or natural law. Human societies have generally acknowledged that unjustified killing is wrong. When they make exceptions for the sake of expediency, they need to be reminded of what the moral law requires. This is true regardless of whether the inquiry concerns the killing of others or of oneself: both involve the taking of an innocent human life, and thus the same standard should be applied to each.
What does such a suggestion yield, if we combine the insights of Cicero and Augustine? Cicero teaches us that the conflict between true expediency and justice is an illusion. Augustine reminds us that killing the innocent is wrong. Physician-assisted suicide is ultimately the killing of the innocent. Therefore, any attempt to justify such an action on the grounds of apparent utility—here represented by two impulses that are good in themselves, that is, compassion and a desire to alleviate suffering—must be found wanting. If suicide is an action that is unjust in itself, no utilitarian arguments in its favor, however rhetorically compelling or seemingly ethical, can transform it into a just action.
The first and most important purpose of the state’s laws is to establish justice, the most basic principle of which is the protection and preservation of life. Canada’s regulations regarding so-called “medical assistance in dying” are fundamentally contrary to this purpose. In a just political order they would be overturned.
Enlarge / A woman watches white flags on the National Mall on September 18, 2021, in Washington, DC. Over 660,000 white flags were installed here to honor Americans who have lost their lives to COVID-19. (credit: Getty | Chen Mengtong)
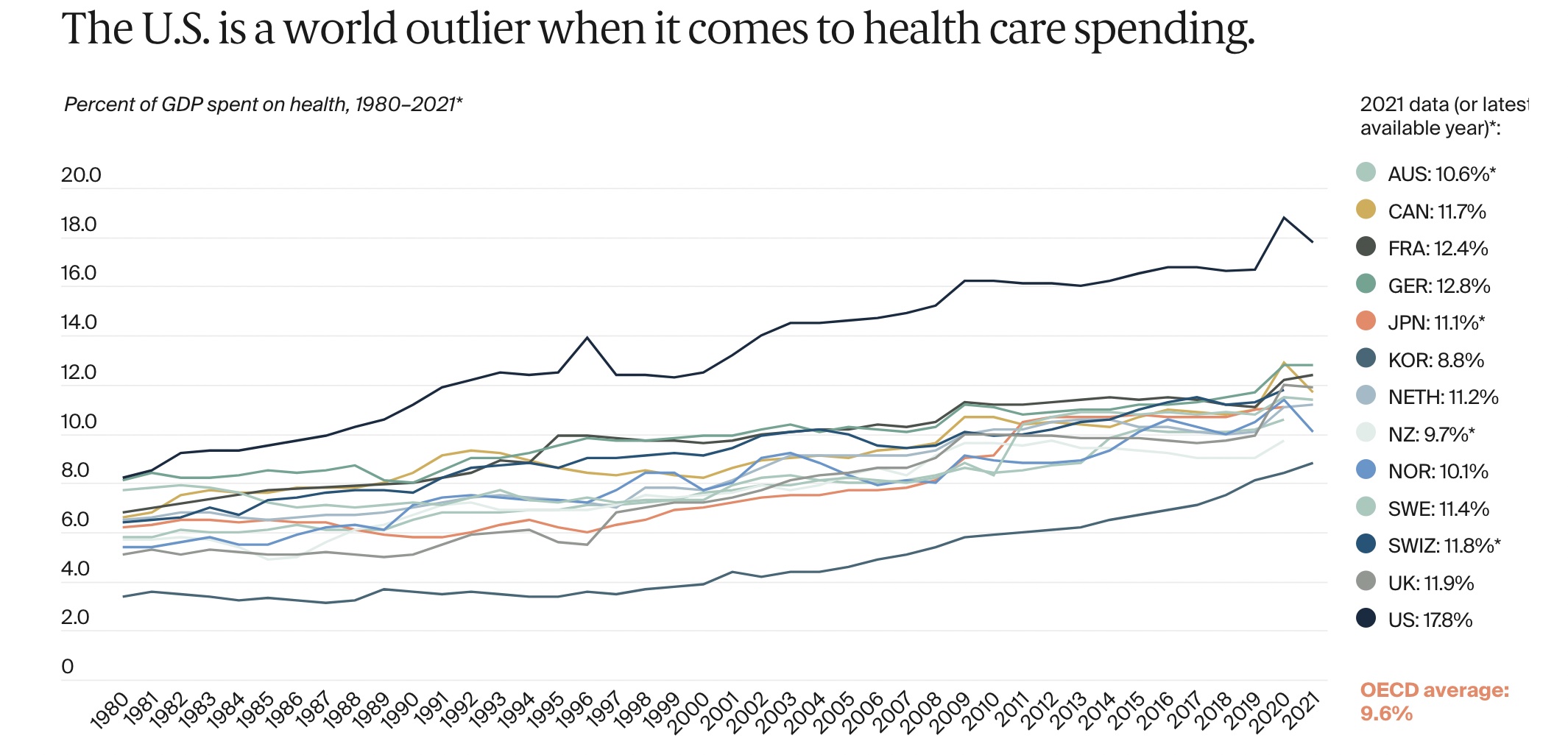
Americans spend an exorbitant amount of money on health care and have for years. As a country, the US spends more on health care than any other high-income country in the world—on the basis of both per-person costs and a share of gross domestic product. Yet, you wouldn't know it from looking at major health metrics in years past; the US has relatively abysmal health. And, if anything, the COVID-19 pandemic only exacerbated the US health care system's failures relative to its peers, according to a new analysis by the Commonwealth Fund.
Compared with other high-income peers, the US has the shortest life expectancy at birth, the highest rate of avoidable deaths, the highest rate of newborn deaths, the highest rate of maternal deaths, the highest rate of adults with multiple chronic conditions, and the highest rate of obesity, the new analysis found.
"Americans are living shorter, less healthy lives because our health system is not working as well as it could be," Munira Gunja, lead author of the analysis and a senior researcher for The Commonwealth Fund’s International Program in Health Policy and Practice Innovation, said in a press statement. "To catch up with other high-income countries, the administration and Congress would have to expand access to health care, act aggressively to control costs, and invest in health equity and social services we know can lead to a healthier population."
{kind=link}